
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Acute Coronary Syndrome (ACS) STEMI ❤️ ✅
Related Subjects: | AP of the Coronary Arteries |Acute Coronary Syndrome: Overview |Atherosclerosis |Ischaemic heart disease |Assessing Chest Pain |Acute Coronary Syndrome (ACS): Complications |ACS - General |ACS - STEMI |ACS - NSTEMI |ACS - GRACE Score |ACS - ECG Changes |Cardiac Troponins |ACS - Post MI arrhythmias |ACS: Right Ventricular STEMI |ACS: Sgarbossa Criteria |Wellen's syndrome
📊 Initial Management of Acute STEMI
| 🫀 STEMI Management - NICE NG185-aligned summary |
|---|
🚑 Immediate actions - do in parallel
NICE sources: NG185 recommendations | NG185 STEMI visual summary |
🫀 Site of Coronary Artery Occlusion in STEMI
- Right coronary artery occlusion
- ST depression in lead I.
- ST elevation in lead III greater than in lead II.
a. Proximal occlusion- ST elevation more than 1 mm with positive T wave in lead V₄R.
b. Distal occlusion- ST isoelectric with a positive T wave in lead V₄R.
- Left circumflex artery occlusion
- ST elevation in lead II greater than lead III.
- ST isoelectric or elevated in lead I.
- ST isoelectric or depressed with negative T wave in V₄R.
a. Extension to posterior wall- ST depression in precordial leads.
b. Extension to lateral wall- ST elevation in leads I, aVL, V₅ and V₆.
- Left anterior descending artery occlusion
a. Proximal to first septal branch and first diagonal branch
- ST elevation in leads aVR and aVL.
- ST depression in leads II, III and aVF.
- ST elevation in lead V₁ >2 mm and leads V₂ to V₄.
- ST isoelectric or depressed in leads V₅ and V₆.
- Acquired intra-Hisian block or RBBB may occur.
b. Distal to first septal branch, proximal to first diagonal branch- ST elevation in leads I and aVL.
- ST depression in lead III, with lead II isoelectric.
- ST elevation in leads V₂ to V₆ but not in lead V₁.
c. Distal to first diagonal branch, proximal to first septal branch- ST depression in aVL, highest in lead III.
- ST elevation in inferior leads, highest in lead III.
- ST elevation in leads V₁ to V₄.
d. Distal LAD- ST depression in aVR.
- ST elevation in inferior leads, highest in lead II.
- ST elevation in leads V₃ to V₆.
- Left main coronary artery occlusion
- ST elevation in lead aVR.
- ST elevation in lead V₁, usually lower than in aVR.
- ST depression in leads II and aVF.
- ST depression in precordial leads to the left of V₂.
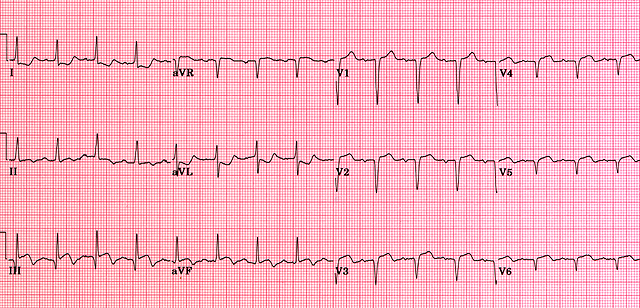
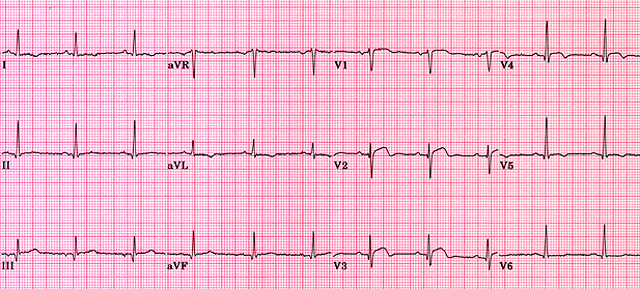
🖼️ STEMI ECG Examples



🫀 Management of Acute STEMI - NICE NG185 + ESC 2023 aligned
🚨 Key principle: STEMI is a time-critical reperfusion emergency. Do not delay reperfusion for CXR, routine bloods or waiting for troponin.
NICE timing logic: offer primary PCI if it can be delivered within 120 minutes of the time fibrinolysis could have been given; otherwise offer fibrinolysis if within 12 hours, appropriate and not contraindicated.
Time = myocardium ⏱️
⚡ Pathophysiology - why speed matters
- Cause: usually plaque rupture or erosion → platelet activation + thrombin generation → acute coronary thrombotic occlusion.
- Wavefront necrosis: infarction spreads from endocardium to epicardium over hours; early reperfusion salvages myocardium and preserves LV function.
- Electrical instability: acute ischaemia increases VT/VF risk early; hence monitoring and defibrillator readiness.
🩺 Clinical features - typical and atypical
- Typical pain: central crushing/tight chest pain lasting >20 minutes, with or without radiation to jaw, left arm, neck or back.
- Associated symptoms: dyspnoea, sweating 😰, nausea/vomiting, palpitations, syncope or sense of doom.
- Atypical presentations: older adults, women, diabetes and CKD may present with dyspnoea, collapse, epigastric discomfort, confusion or minimal pain.
- Examination clues: hypotension/shock, pulmonary oedema, new pansystolic murmur, bradycardia in inferior/RV MI, or arrhythmia.
📉 ECG diagnosis - STEMI and STEMI equivalents
- ST elevation in ≥2 contiguous leads supports STEMI when consistent with symptoms and clinical context.
- V2–V3: use sex/age-specific thresholds; commonly ≥2 mm in men and ≥1.5 mm in women, with higher thresholds often used in younger men.
- Other leads: ≥1 mm ST elevation in at least 2 contiguous leads.
- Posterior MI: ST depression V1–V3 with tall R waves → record V7–V9; posterior ST elevation supports STEMI pathway.
- Right ventricular MI: consider with inferior STEMI + hypotension → record V3R/V4R; avoid nitrates if RV infarct suspected.
- LBBB or paced rhythm: new LBBB alone is not diagnostic, but ischaemic symptoms with concordant ST changes or strong clinical suspicion should trigger urgent senior/cardiology review and possible STEMI pathway activation.
- Repeat ECGs: repeat if symptoms persist or evolve because dynamic STEMI can be missed on the first trace.
🧪 Troponin - do not wait for it
- Troponin supports diagnosis and risk assessment, but STEMI is a clinical + ECG diagnosis requiring immediate reperfusion when clear.
- High-sensitivity troponin may be normal early, so a normal initial troponin does not exclude acute coronary occlusion.
- Bedside echo can help if the diagnosis is unclear, for example regional wall motion abnormality, but should not delay reperfusion when STEMI is clear.
🚑 Immediate actions - first 5–10 minutes
- ABCDE, activate cath lab / STEMI pathway early, and involve a senior decision-maker.
- Cardiac monitor + defibrillator ready ⚡; treat VT/VF according to ALS.
- 12-lead ECG and repeat if evolving; consider posterior and right-sided leads when indicated.
- IV access x2, point-of-care glucose and bloods, but do not delay reperfusion.
- Oxygen only if hypoxaemic: target 94–98%, or 88–92% if at risk of hypercapnic respiratory failure.
- Do not delay reperfusion for CXR unless there is strong suspicion of aortic dissection or another diagnosis requiring immediate imaging.
💊 Symptom relief - analgesia and anti-ischaemic treatment
- Opioid analgesia: IV morphine or diamorphine titrated to pain, plus antiemetic such as metoclopramide or ondansetron if needed.
- GTN: sublingual or IV for ongoing pain and hypertension if no contraindications.
- Avoid GTN in hypotension, suspected RV infarct, severe aortic stenosis or recent PDE5 inhibitor use.
- Positioning: upright if pulmonary oedema; supine/legs elevated if hypotensive while treating shock.
🩸 Antiplatelet therapy - NICE NG185
✅ Core: aspirin + a P2Y12 inhibitor. NICE specifies prasugrel + aspirin for STEMI undergoing primary PCI in people not already taking an oral anticoagulant, with age, weight and bleeding cautions.
- Aspirin: 300 mg loading dose as soon as possible, chewed/crushed if needed, then 75 mg daily long-term unless contraindicated.
- If primary PCI is planned and not on oral anticoagulant: offer prasugrel + aspirin.
- Prasugrel cautions: avoid if previous stroke/TIA; consider alternatives if age ≥75 years, body weight <60 kg, frailty or high bleeding risk.
- If prasugrel is unsuitable, consider ticagrelor or clopidogrel with aspirin according to cardiology/local pathway.
- If already taking an oral anticoagulant: offer clopidogrel + aspirin.
- If STEMI is not treated with PCI: offer ticagrelor + aspirin unless bleeding risk is high; if high bleeding risk, consider clopidogrel + aspirin or aspirin alone. If fibrinolysis is used, follow the local fibrinolysis protocol for the immediate P2Y12 choice and timing.
🧬 Antithrombin / anticoagulation - match to strategy
- Primary PCI with radial access: offer UFH with bailout glycoprotein IIb/IIIa inhibitor.
- If femoral access is needed: consider bivalirudin with bailout glycoprotein IIb/IIIa inhibitor.
- If fibrinolysis is given: give an antithrombin at the same time, according to local protocol.
- Avoid routine pre-hospital fibrinolysis or routine GP IIb/IIIa inhibitor use when primary PCI is planned.
- Renal function: adjust dosing where relevant and monitor bleeding risk closely.
⚡ Reperfusion strategy - NICE NG185 + ESC 2023 framing
- Primary PCI preferred: offer coronary angiography with follow-on primary PCI if indicated when presentation is within 12 hours of symptom onset and primary PCI can be delivered within 120 minutes of the time fibrinolysis could have been given.
- Fibrinolysis: offer if within 12 hours, timely primary PCI is not achievable, and there are no contraindications to fibrinolysis.
- Cardiogenic shock: offer urgent coronary angiography with follow-on PCI if indicated; consider even after 12 hours if ongoing ischaemia or shock persists.
- Late presenters >12 hours: consider angiography/PCI if ongoing ischaemia, haemodynamic instability, malignant arrhythmias or shock.
- System delay: where possible, bypass non-PCI centres and move directly to cath lab in confirmed STEMI.
💉 If fibrinolysis is used - what next?
- Give antithrombin at the same time as fibrinolysis.
- Repeat ECG at 60–90 minutes after fibrinolysis.
- Failed reperfusion: persistent ST elevation or ongoing pain → offer immediate coronary angiography with follow-on PCI if indicated; do not repeat fibrinolysis.
- Recurrent ischaemia: seek urgent cardiology advice and consider angiography/PCI.
- Successful fibrinolysis and stable: consider angiography during the same admission.
🩻 Cath lab / in-hospital strategy - NICE NG185
- Access: radial preferred when feasible.
- Stent choice: offer drug-eluting stent if stenting is indicated.
- Thrombus management: thrombus aspiration may be considered during primary PCI, but mechanical thrombus extraction should not be used routinely.
- Multivessel disease:
- If no shock: offer complete revascularisation, often during index admission or staged.
- If cardiogenic shock: consider culprit-only revascularisation during the index procedure.
- LV function: assess LV function in all STEMI patients, ideally before discharge or in early follow-up.
🧠 Special situations - high yield
- Inferior STEMI + hypotension: think RV infarct; record right-sided leads; avoid nitrates; treat with cautious fluids and urgent reperfusion.
- Posterior MI: record V7–V9; treat as STEMI equivalent if posterior ST elevation is present.
- Cardiac arrest with ROSC: if ECG/clinical picture suggests acute coronary occlusion, urgent cath lab discussion is warranted according to local network protocol.
- Suspected aortic dissection: tearing pain radiating to back, pulse/BP differential, new aortic regurgitation murmur or mediastinal widening → avoid anticoagulants/thrombolysis and image urgently.
💓 Beta-blockers, ACEi/ARB, MRA - inpatient and discharge
- ACE inhibitor / ARB: start when haemodynamically stable, especially with LV dysfunction, anterior MI, diabetes, hypertension or CKD; titrate to target doses.
- Beta-blocker: offer after MI unless contraindicated; particularly important with LV dysfunction, heart failure, arrhythmia or ongoing angina. Avoid or withhold in shock, acute pulmonary oedema, severe bradycardia, heart block or severe asthma.
- Aldosterone antagonist, e.g. eplerenone: consider if LVEF ≤40% with heart failure or diabetes after MI; monitor potassium and renal function closely.
- High-intensity statin: start early unless contraindicated and continue long-term.
🩹 Secondary prevention - what saves lives long-term
- DAPT: aspirin + P2Y12 inhibitor as directed, often up to 12 months; shorter if bleeding risk high, longer only in selected high-ischaemic-risk cases under specialist advice.
- Statin: high-intensity statin long-term; consider add-on lipid therapy in very high-risk patients if targets are not met.
- BP, diabetes, smoking: aggressive risk factor control; smoking cessation has one of the largest absolute benefits.
- Cardiac rehab: structured rehab improves outcomes and adherence; include exercise prescription, education and psychosocial support.
- Vaccination: influenza and other vaccinations according to risk group/local policy to reduce infection-triggered events.
📅 Inpatient monitoring and complications to watch for
- Arrhythmias: VT/VF early; AF; bradyarrhythmias in inferior MI; monitor and treat according to ALS/cardiology guidance.
- Heart failure / pulmonary oedema: diuretics, nitrates if BP allows, ventilatory support if needed, and assess LVEF.
- Mechanical complications, often 2–7 days: papillary muscle rupture causing acute MR, VSD, free wall rupture causing tamponade; suspect if sudden shock or new murmur.
- Pericarditis: pleuritic pain and pericardial rub early; Dressler syndrome later.
📊 Risk stratification - use the right tools
- Reperfusion decisions in STEMI are ECG + time + clinical status driven, not primarily GRACE/TIMI driven.
- After reperfusion, prognosis is guided by:
- Killip class / heart failure severity.
- LVEF on echo.
- Extent of coronary disease and success of revascularisation.
- Bleeding risk, renal function, frailty and complications during admission.
- GRACE is primarily a NSTEMI/unstable angina risk tool and is not the main determinant for acute STEMI reperfusion.
💡 Teaching pearl: A normal early troponin does not exclude STEMI. The life-saving decision is whether the ECG and clinical picture require immediate reperfusion. STEMI is a coronary occlusion problem first; troponin is confirmatory, but reperfusion is therapeutic.
🧠 Pathophysiology pearl: STEMI usually occurs when plaque rupture or erosion triggers platelet-rich thrombus and complete coronary occlusion. Myocardial necrosis spreads as a wavefront from subendocardium to epicardium, so every delay reduces salvageable myocardium. This is why the pathway prioritises rapid ECG recognition, antithrombotic therapy and immediate reperfusion.
📚 References - guidelines
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery