
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Multiple Myeloma
Related Subjects: |Hypercalcaemia |Multiple Myeloma |Extramedullary Plasmacytoma |Smouldering Myeloma |MGUS |Waldenstrom Macroglobulinaemia |Oncological emergencies
🔎 Always think of myeloma in a patient with bone pain, raised calcium, or an unexplained high ESR.
📘 About
- Malignant tumour of plasma cells (B-cell lineage).
- Produces monoclonal immunoglobulin (usually IgG or IgA) or light chains (Bence–Jones proteins).
- Median survival ~2–3 years (improving with newer therapies).
- >MGUS (Monoclonal Gammopathy of Undetermined Significance) can develop into MM
📊 Incidence
- ~5,500 new cases per year in the UK 🇬🇧.
- Incidence ~5.4/100,000/year; more common in men.
- Twice as common in patients of African descent.
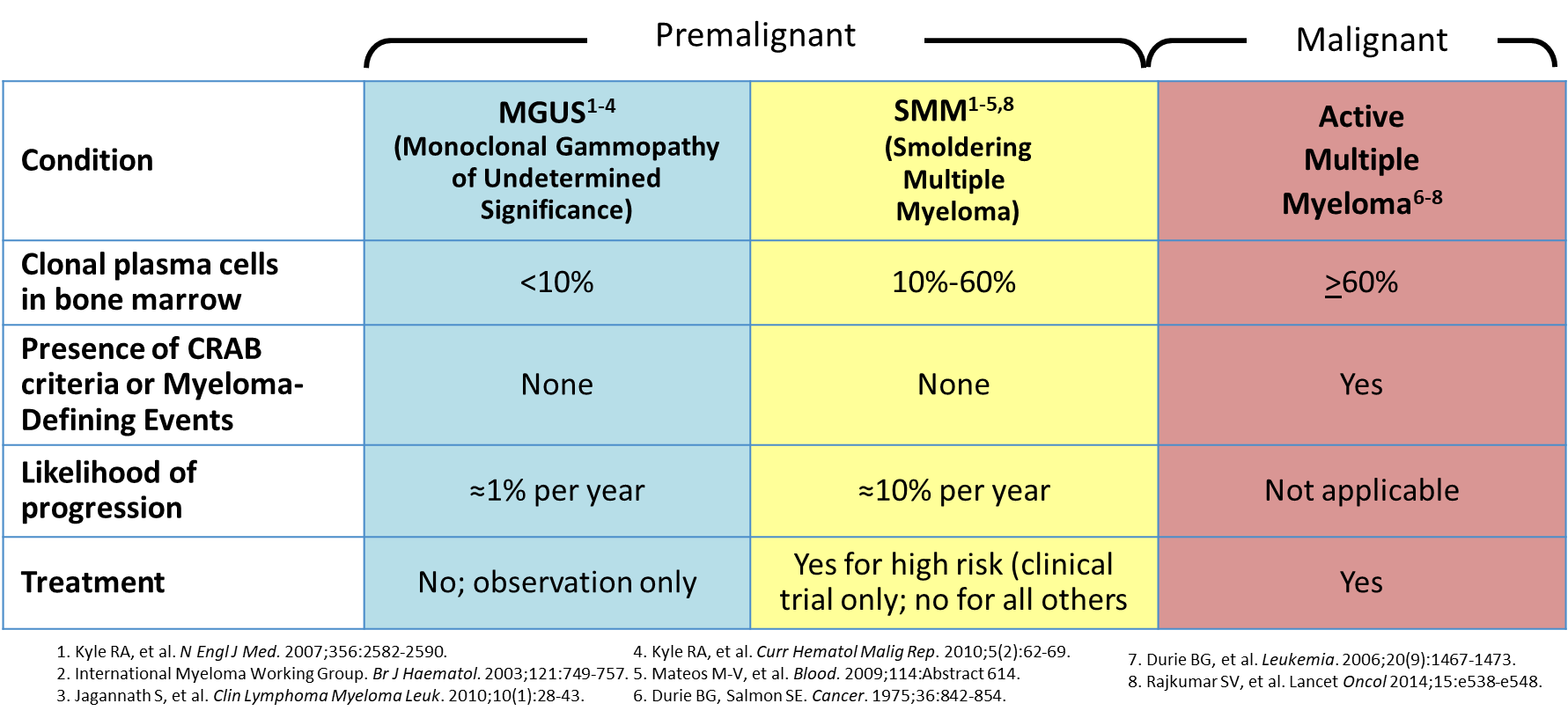
📈 Spectrum of Plasma Cell Disorders
- MGUS: Asymptomatic, low paraprotein, no organ damage. ~1% per year go to myeloma. Monitoring only 🩺.
- Smouldering Myeloma: Higher paraprotein and marrow plasma cells, but still no CRAB features. Close observation 👀.
- Multiple Myeloma: Full-blown disease with monoclonal protein + ≥1 CRAB feature (end-organ damage).
💡 CRAB = HyperCalcaemia, Renal impairment, Anaemia, Bone lesions.
⚙️ Aetiology & Pathophysiology
- Uncontrolled plasma cell clone infiltrates marrow → cytopenias.
- Secretion of abnormal immunoglobulins → hyperviscosity & renal failure.
- Suppression of normal immunoglobulins → immunodeficiency 🔻.
- Plasma cell proteins stimulate osteoclasts → lytic bone disease & fractures 🦴.
- Light chains damage kidneys → cast nephropathy.
🧑⚕️ Clinical Features
- Age >60, male > female.
- Bone pain (esp. back, ribs, skull); vertebral collapse → cord compression.
- Renal impairment (light chain nephropathy).
- Infections due to low normal immunoglobulins (immunoparesis).
- Anaemia → fatigue, pallor.
- Hypercalcaemia → thirst, confusion, constipation.
- AL Amyloidosis: neuropathy, restrictive cardiomyopathy, nephrotic syndrome, macroglossia 👅.
- Hyperviscosity syndrome (IgA myeloma): blurred vision, headaches, bleeding.
🧪 Investigations
- FBC: Normocytic anaemia, cytopenias. Rouleaux formation (High ESR)
- Biochemistry: ↑ ESR, ↑ calcium, ↑ urate, ↑ LDH.
- Renal function: may show AKI or CKD.
- Serum protein electrophoresis & urine for BJP: Monoclonal paraprotein.
- Serum free light chain assay
- Bone marrow aspirate/biopsy: >10% clonal plasma cells; FISH for cytogenetics.
- Imaging: Whole-body MRI, CT or PET-CT for lytic lesions. Skull: Lytic lesions. Raindrop skull X-ray
- Prognosis: β2-microglobulin ↑ = poor prognosis.
🩸 CRAB Mnemonic
- 🟠 Hypercalcaemia: Ca²⁺ >2.75 mmol/L.
- 🟣 Renal failure: CrCl <40 ml/min or creatinine >177 µmol/L.
- 🔴 Anaemia: Hb <100 g/L.
- ⚫ Bone lesions: lytic lesions, fractures, osteoporosis.
🚑 Complications
- Pathological fractures & spinal cord compression.
- Hypercalcaemia crisis.
- Renal failure (cast nephropathy).
- Recurrent infections (esp. pneumonia, sepsis).
- Pancytopenia & bleeding.
- Amyloidosis(AL)
💊 Management
- Fit / Younger Patients: Bortezomib + thalidomide + dexamethasone → autologous stem cell transplant (ASCT).
- Supportive: Transfusions, bisphosphonates (zoledronate/pamidronate) for bone disease, hydration for hypercalcaemia.
- Pain management: Analgesics, radiotherapy for focal lesions.
- Hyperviscosity: Plasma exchange if symptomatic.
- Prophylaxis: Vaccinations, antibiotics, allopurinol for hyperuricaemia.
- Palliative: Discuss prognosis, goals of care, symptom management.
📌 Key exam pearl: If you see “elderly patient + back pain + renal impairment + hypercalcaemia + raised ESR” → think myeloma until proven otherwise 🚨.
Cases - Multiple Myeloma
- Case 1 - Bone pain & lytic lesions 🦴: A 68-year-old man presents with persistent back pain and fatigue. Exam: spinal tenderness. Bloods: normocytic anaemia, calcium 3.1 mmol/L, creatinine 160 µmol/L. X-ray: “punched-out” lytic lesions in vertebrae. Serum electrophoresis: monoclonal IgG spike. Diagnosis: multiple myeloma with bone disease. Managed with bisphosphonates, chemotherapy (bortezomib/lenalidomide/dexamethasone), and supportive care.
- Case 2 - Renal impairment 🩺: A 72-year-old woman is admitted with confusion and oliguria. Bloods: urea 25 mmol/L, creatinine 480 µmol/L, calcium 2.7 mmol/L. Urine: Bence–Jones proteinuria. Renal biopsy: light chain cast nephropathy. Diagnosis: myeloma kidney. Managed with hydration, chemotherapy, and dialysis if required.
- Case 3 - Recurrent infections 🦠: A 61-year-old man has recurrent pneumonias and sinusitis. Bloods: IgG low, Hb 9.5 g/dL, raised ESR. Serum electrophoresis: monoclonal IgA band. Bone marrow: 20% plasma cells. Diagnosis: multiple myeloma with immunoparesis. Managed with chemotherapy, immunoglobulin replacement, and infection prophylaxis.
Teaching Point 🩺: Multiple myeloma is a malignant plasma cell disorder producing monoclonal immunoglobulins. Classic features = CRAB: - Calcium ↑ (hypercalcaemia) - Renal impairment - Anaemia - Bone lesions Diagnosis requires serum/urine electrophoresis, free light chain assay, and bone marrow biopsy. Treatment = chemotherapy, bisphosphonates, and supportive care.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery