Spinal Cord Infarction
Related Subjects:
|Neurological History taking
|Motor Neuron Disease (MND-ALS)
|Miller-Fisher syndrome
|Guillain Barre Syndrome
|Multifocal Motor Neuropathy with Conduction block
|Inclusion Body Myositis
|Multiple Sclerosis (MS) Demyelination
|Transverse myelitis
|Acute Disseminated Encephalomyelitis
|Cervical spondylosis
|Spinal Cord Anatomy
|Acute Disc Prolapse
|Spinal Cord Compression
|Spinal Cord Haematoma
|Foix-Alajouanine syndrome
|Cauda Equina
|Conus Medullaris syndrome
|Anterior Spinal Cord syndrome
|Central Spinal Cord syndrome
|Brown-Sequard Spinal Cord syndrome
|Vitamin B12 deficiency
|Myelopathy
|Spinal Cord Arteriovenous Malformations
📖 About
- 🧠 Spinal cord infarction is a rare but severe cause of acute myelopathy, most often linked to aortic disease or surgery.
- ⚡ Classically presents as Anterior Spinal Artery Syndrome.
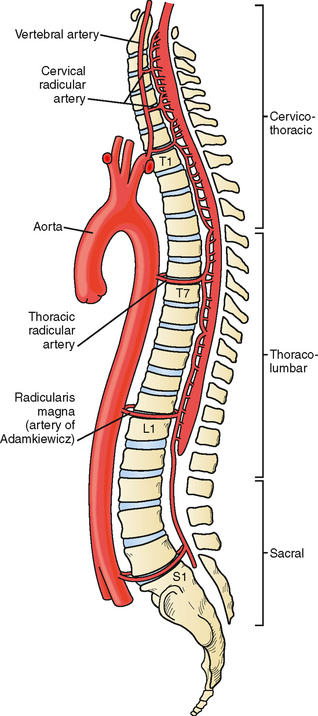
🩸 Vascular Supply
- Anterior Spinal Artery: Single vessel supplying anterior 2/3 of cord (motor tracts + spinothalamic pathways).
- Posterior Spinal Arteries: Paired vessels supplying posterior 1/3 (dorsal columns).
- Segmental Arteries: Aortic branches reinforce supply - most important is the Artery of Adamkiewicz (T6–L4), critical for lower cord perfusion.
- 🟡 The mid-thoracic cord is especially vulnerable → “watershed” zone with poor collateral supply.
🧩 Anatomy
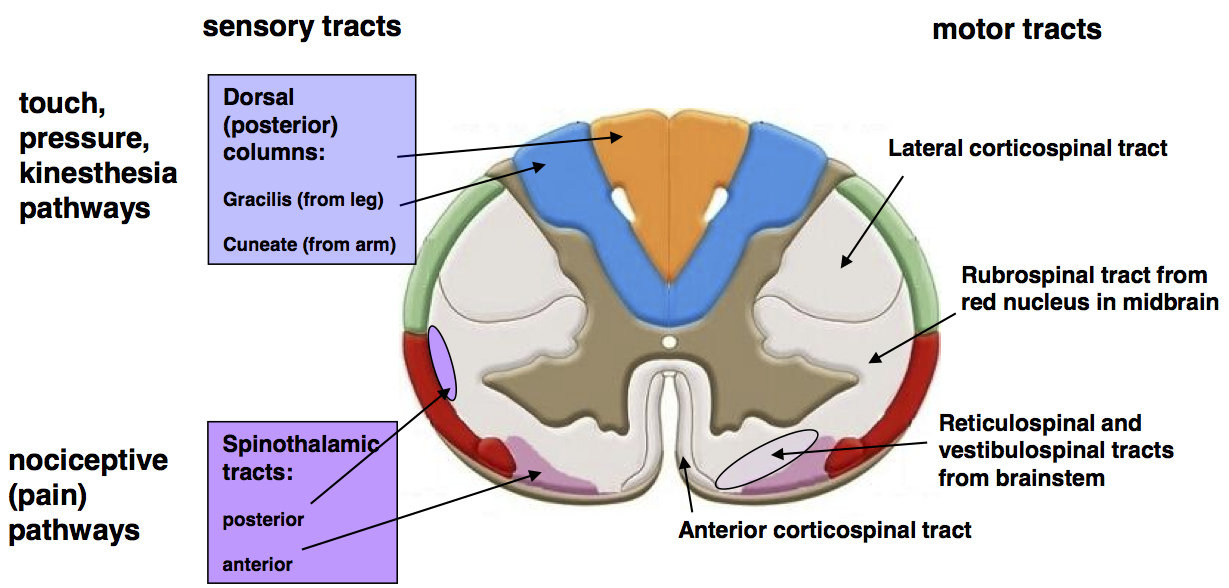
🧩 Cross Section
⚠️ Aetiology
- 🩻 Thoraco-abdominal aortic dissection.
- 🔪 Aortic aneurysm repair or cross-clamping.
- 🧪 Atherosclerotic vessel occlusion.
- 💔 Embolic events (e.g., atrial fibrillation, atheroembolism).
- Rare: systemic hypotension, vasculitis, coagulopathy.
🔬 Pathophysiology
- 🟥 Infarction typically affects anterior 2/3 of cord (corticospinal + spinothalamic tracts + anterior horn cells).
- 🟦 Posterior columns are spared → vibration & proprioception intact.
- “Disconnection syndrome”: profound motor and pain/temperature loss but preserved dorsal column sensation.
🩺 Clinical Presentation
- ♿ Sudden onset flaccid paraplegia → later spasticity.
- 🚽 Loss of bladder and bowel control.
- 🔥 Loss of pain and temperature sensation below lesion.
- 🎯 Preservation of vibration and proprioception (posterior column sparing).
- Onset often abrupt during/after aortic surgery or severe hypotension.
🚨 Red Flag: Sudden paraplegia following aortic surgery or dissection = spinal cord infarction until proven otherwise. Requires urgent MRI and vascular input.
🧪 Investigations
- 🖥 MRI spine (incl. diffusion-weighted) = most sensitive; may show “pencil-like” T2 hyperintensity.
- CT spine if MRI unavailable.
- 🩸 Bloods: screen for vascular risk (lipids, glucose, clotting, vasculitis screen if indicated).
- 🩻 CT or MR angiography → assess aortic and segmental vessel supply.
💊 Management
- Supportive Care: ABCs, oxygen, cardiovascular stabilisation.
- Pressure Care: Prevent sores with regular repositioning.
- Bowel/Bladder Management: Catheterisation, bowel regimen.
- VTE Prophylaxis: LMWH, stockings.
- Rehabilitation: Early physio, OT, mobility aids to maximise independence.
- Prevention: Careful aortic surgery technique, maintain cord perfusion pressure, avoid hypotension.
