Related Subjects: Atropine
|Acute Anaphylaxis
|Basic Life Support
|Advanced Life Support
|Adrenaline/Epinephrine
|Acute Hypotension
|Cardiogenic shock
|Distributive Shock
|Hypovolaemic or Haemorrhagic Shock
|Obstructive Shock
|Septic Shock and Sepsis
|Shock (General Assessment)
|Toxic Shock Syndrome
🫀 Transcutaneous pacing (TCP) is a rapid, non-invasive method of providing temporary cardiac pacing in patients with severe symptomatic bradyarrhythmias.
It is usually used as an emergency bridge to transvenous pacing or definitive treatment. TCP poses no electrical risk to staff, and CPR can continue if required.
Always follow the ALS Bradycardia Algorithm.
ℹ️ What is transcutaneous pacing?
- TCP delivers electrical impulses through external defibrillator pads to stimulate myocardial depolarisation and ventricular contraction.
- It is used when bradycardia is causing serious compromise, such as hypotension, syncope, shock, myocardial ischaemia or heart failure.
- It can be life-saving, but it is often painful because skeletal muscle is stimulated as well as the heart.
- Give analgesia and sedation if the patient is conscious and the clinical situation allows.
- TCP is usually a temporary bridge while treating reversible causes or arranging transvenous pacing.
⚠️ When to consider TCP
- Severe symptomatic bradycardia not responding to initial treatment.
- High-risk conduction disease, such as complete heart block with instability.
- Bradycardia with adverse features: shock, syncope, myocardial ischaemia or heart failure.
- Failure or delay in response to atropine or chronotropic drugs.
🔍 Check reversible causes
- Hypoxia 🫁
- Hyperkalaemia ⚡
- Drug toxicity, especially beta-blockers, calcium-channel blockers, digoxin or opioids 💊
- Hypothermia ❄️
- Myocardial infarction or ischaemia 🫀
- Raised vagal tone or vasovagal episodes.
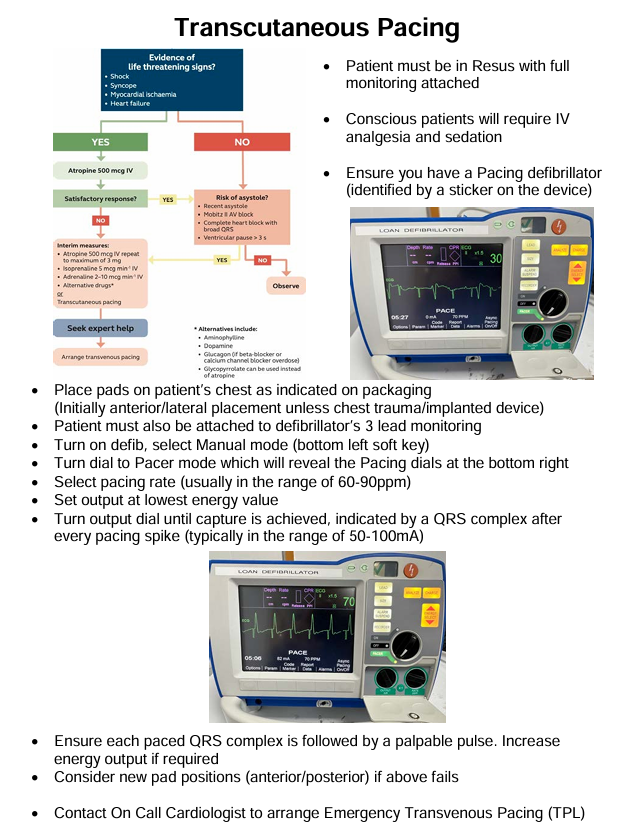
🧰 Method
- Apply defibrillator pads and select pacing mode.
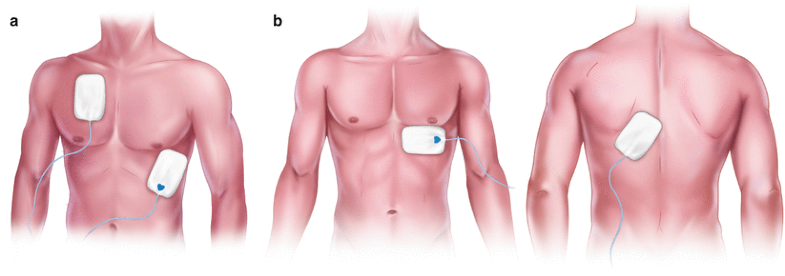
- Preferred pad position:
- Anterior pad over the cardiac apex or V3 region.
- Posterior pad below the left scapula.
- Alternative position: standard anterior-lateral defibrillation position.
- Keep pads away from implanted pacemakers or ICDs.
- Remove transdermal drug patches before applying pads.
- Prepare the skin: dry the chest and shave excess hair if needed.
- Attach ECG monitoring, blood pressure monitoring and pulse oximetry.
- Give oxygen if hypoxic and obtain IV access.
- Give analgesia and sedation if conscious, for example titrated IV opioid and benzodiazepine according to local policy.
⚙️ Typical settings
- Rate: usually 60–80 bpm; 70 bpm is commonly used.
- Output current: start low and increase gradually until capture is achieved.
- Typical output range is around 20–120 mA, but higher outputs may occasionally be required.
- Pulse duration: commonly around 20–40 ms, depending on the device.
- Once capture is achieved, increase the output slightly above threshold to maintain reliable pacing.
✅ Confirm capture
- Electrical capture: pacing spike followed immediately by a broad QRS complex and T wave.
- Mechanical capture: a corresponding palpable pulse, improved blood pressure or improved perfusion.
- Do not rely on the monitor alone - muscle twitching can mimic a pulse.
- Continue monitoring BP, SaO₂, ECG rhythm, conscious level and pain.
🚨 If capture fails
- Increase the pacing output.
- Check pad contact and cable connections.
- Reposition the pads, preferably to an anterior-posterior position.
- Reduce skin impedance by drying the skin and improving pad contact.
- Treat reversible causes, especially hyperkalaemia, hypoxia and drug toxicity.
- Arrange urgent expert help and consider transvenous pacing.
💡 Clinical pearls
- TCP is fast, temporary and uncomfortable.
- It is particularly useful when the patient is unstable and definitive pacing is not immediately available.
- The aim is not just a paced ECG trace - the patient needs mechanical capture and clinical improvement.
- In conscious patients, pain relief is important because chest wall muscle contraction can be distressing.
- Exam phrases to remember: “bridge to definitive pacing”, “confirm mechanical capture” and “treat reversible causes”.
Further details