Acute Anaphylactoid Reactions
Related Subjects: Atropine
|Acute Anaphylaxis
|Basic Life Support
|Advanced Life Support
|Adrenaline (Epinephrine)
|Acute Hypotension
|Cardiogenic shock
|Distributive Shock
|Hypovolaemic or Haemorrhagic Shock
|Obstructive Shock
|Septic Shock and Sepsis
|Shock (General Assessment)
|Toxic Shock Syndrome
⚡ Emergency Reminder: In suspected anaphylaxis give Adrenaline (Epinephrine) immediately.
Dose: 0.5–1 mg (0.5–1 mL of 1:1000) IM into the lateral thigh using a long needle to reach muscle.
💉 Adrenaline is life-saving – do not delay for IV access or investigations.
| 🚑 Initial Management Summary |
|---|
- 📞 Call for senior/anaesthetic help early.
- 🛑 Remove allergen (stop drug or blood transfusion).
- 💨 High-flow oxygen (15 L/min) & maintain airway; patient flat unless severe dyspnoea.
- 💉 Adrenaline (IM 1:1000) into lateral thigh:
- Adult / child >12 yr: 0.5 mL (0.5 mg)
- Child 6–12 yr: 0.3 mL (0.3 mg)
- Child <6 yr: 0.15 mL (0.15 mg)
- ⏱️ Repeat every 5 min if no improvement.
- 💧 IV fluids: Adults 500–1000 mL rapid bolus (0.9% NaCl); children 20 mL/kg.
- 📝 Adjuncts (not first-line in UK/Resus Council guidelines, but often used):
- Hydrocortisone 200 mg IM/slow IV
- Chlorphenamine 10 mg IM/slow IV
- Salbutamol (Albuterol) 5 mg neb if wheeze; escalate if refractory
|

🔎 About
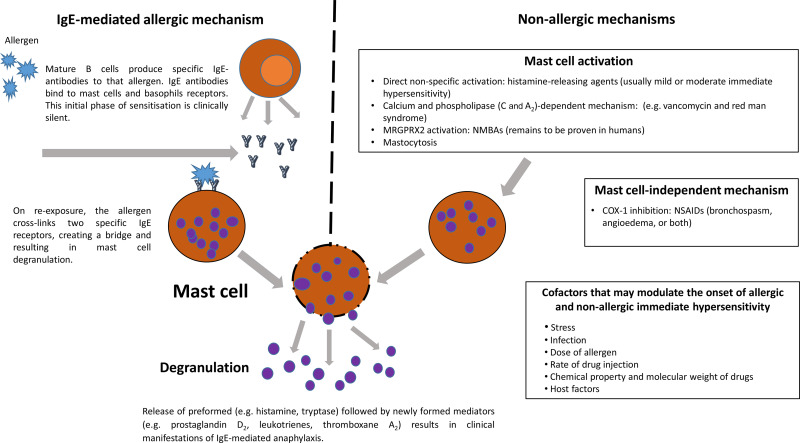
- These reactions resemble acute anaphylaxis but are non–IgE mediated.
- Unlike true allergy, risk does not increase with repeat exposure.
- Some drugs may be cautiously reintroduced if essential (e.g. acetylcysteine in paracetamol overdose).
🧬 Aetiology (Pathophysiology)
- No cross-linking of IgE antibodies on mast cells.
- Instead there is direct mast cell degranulation → histamine & mediator release.
- This explains why skin, gut, and cardiovascular features look identical to IgE reactions.
💊 Common Causative Agents
- Opiates (e.g. morphine)
- Aspirin & NSAIDs
- Acetylcysteine (Parvolex)
- Radiocontrast media (CT, angiography)
- Exercise, cold-induced reactions
🩺 Clinical
- Indistinguishable from IgE anaphylaxis: urticaria, hypotension, bronchospasm, GI upset.
- Key learning point: manage identically in the acute phase.
🔬 Investigations
- ⬆️ Raised mast cell tryptase (peaks at 1–2 hrs, supports diagnosis).
- ❌ Negative specific IgE tests (helps differentiate from true allergy).
🛠️ Management
- 💉 Same acute management as anaphylaxis – adrenaline is first line.
- ✅ Once stabilised, careful review: drug may be restarted under supervision if essential.
- 📋 Always document the event and advise patient about future precautions.
