Oxygen delivery devices
Oxygen therapy is a cornerstone treatment for hypoxaemia and acute respiratory compromise.
Its aim is to improve arterial oxygenation, maintain tissue perfusion, and prevent hypoxic organ injury.
In clinical practice, oxygen is a drug and must be prescribed with a documented target saturation range.
🩺 OSCE Principle: Always state the target saturation before applying oxygen.
⚠️ Hypoxia is life-threatening, but hyperoxia can also cause harm.
FiO₂ depends on device type, flow rate, and the patient’s respiratory effort.
Fixed-performance devices (e.g. Venturi masks) provide more predictable FiO₂ than variable devices.
🗣️ How to Start Oxygen in an OSCE (Step-by-Step)
- Introduce yourself and confirm patient identity.
- Assess Airway and Breathing (A–E approach).
- Check current SpO₂ and respiratory rate.
- State target saturation:
- 94–98% for most patients
- 88–92% if risk of CO₂ retention (e.g. COPD)
- Select appropriate device based on severity.
- Apply oxygen and reassess saturations within minutes.
- Document device, flow rate, target range, and response.
📌 Indications for Oxygen Therapy
- Hypoxaemia (SpO₂ below target range)
- Acute myocardial infarction with hypoxia
- Severe trauma or shock
- Post-anaesthesia recovery
- Acute severe asthma
- Acute pulmonary oedema
- ARDS
- Pneumothorax (accelerates air reabsorption)
- Hypoxic sickle cell crisis
- Cluster headache (high-flow oxygen)
- Carbon monoxide poisoning (100% oxygen)
⚠️ Precautions & Complications
- CO₂ retention (COPD): Excess oxygen may worsen hypercapnia → target 88–92%
- Absorption atelectasis: Prolonged FiO₂ >60%
- Oxygen toxicity: Free radical lung injury with sustained FiO₂ >50%
- Premature infants: Retinopathy of prematurity
- Fire risk: Oxygen-rich environments increase combustion
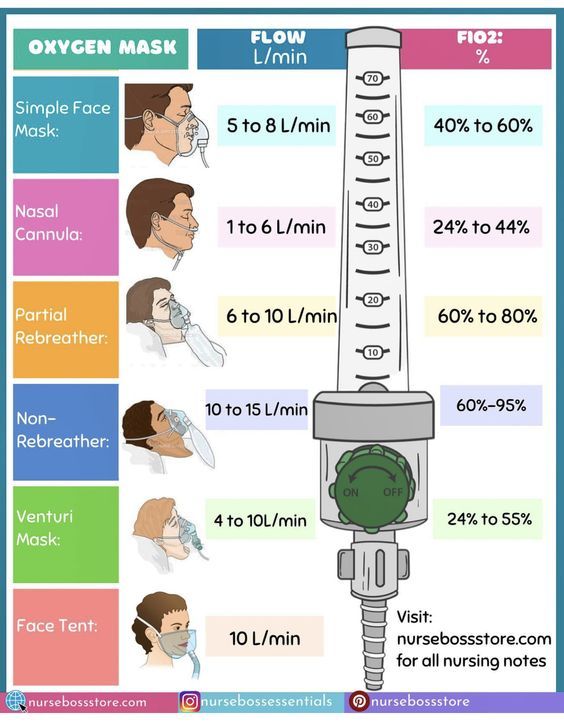
💡 Oxygen Delivery Devices
- 👃 Nasal Cannula: 1–6 L/min → FiO₂ 24–44%. Mild hypoxaemia. Comfortable and allows eating/speaking.
- 😷 Simple Face Mask (Hudson): 5–10 L/min → FiO₂ 40–60%. Avoid <5 L/min (CO₂ rebreathing risk).
- 🎨 Venturi Mask: Fixed FiO₂ 24–60% (colour-coded). Essential for COPD or CO₂ retainers.
- 🫁 Non-Rebreather Mask: 10–15 L/min → FiO₂ 60–90%. Severe hypoxaemia. Reservoir bag must remain inflated.
- 🌬️ High-Flow Nasal Cannula (HFNC): Up to 60 L/min humidified oxygen. Reduces work of breathing.
- ✋ Bag-Valve Mask (BVM): With reservoir → ~100% FiO₂. Used in respiratory arrest/peri-arrest.
- 🫀 CPAP: Continuous positive airway pressure. Indications: acute pulmonary oedema, Type I respiratory failure, OSA.
- 🔄 BiPAP (NIV): IPAP/EPAP pressures. Indications: COPD exacerbation (Type II RF), neuromuscular weakness.
🎯 Target Oxygen Saturations
- Most acutely unwell: 94–98%
- Risk of CO₂ retention: 88–92%
- Titrate oxygen to target and reassess frequently.
📊 Summary Table
| Device |
Flow (L/min) |
Approx. FiO₂ |
Clinical Use |
| Room Air | – | 21% | Stable, no hypoxaemia |
| Nasal Cannula | 1–6 | 24–44% | Mild hypoxia |
| Simple Mask | 5–10 | 40–60% | Moderate hypoxia |
| Venturi Mask | Fixed | 24–60% | Controlled oxygen (COPD) |
| Non-Rebreather | 10–15 | 60–90% | Severe hypoxia |
| HFNC | Up to 60 | Up to 100% | Severe distress |
| BVM | 15 | ~100% | Respiratory arrest |
| CPAP / BiPAP | Variable | Variable | Type I / II RF |
| Colour |
Flow (L/min) |
FiO₂ |
| Blue |
2–4 |
24% |
| White |
4–6 |
28% |
| Yellow |
8–10 |
35% |
| Red |
10–12 |
40% |
| Green |
12–15 |
60% |
🩺 OSCE Viva Tips
- Always use an A–E approach before focusing only on oxygen.
- Explain why you chose that device.
- Mention target saturation explicitly.
- Reassess and escalate if SpO₂ does not improve.
- Consider ABG if worsening or risk of CO₂ retention.
📚 References
- British Thoracic Society Guideline for Oxygen Use in Adults (2022)
- NICE Guidance: Oxygen Therapy
- WHO Oxygen Therapy Manual
