
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Pancoast tumour (Cancer)
🧾 About
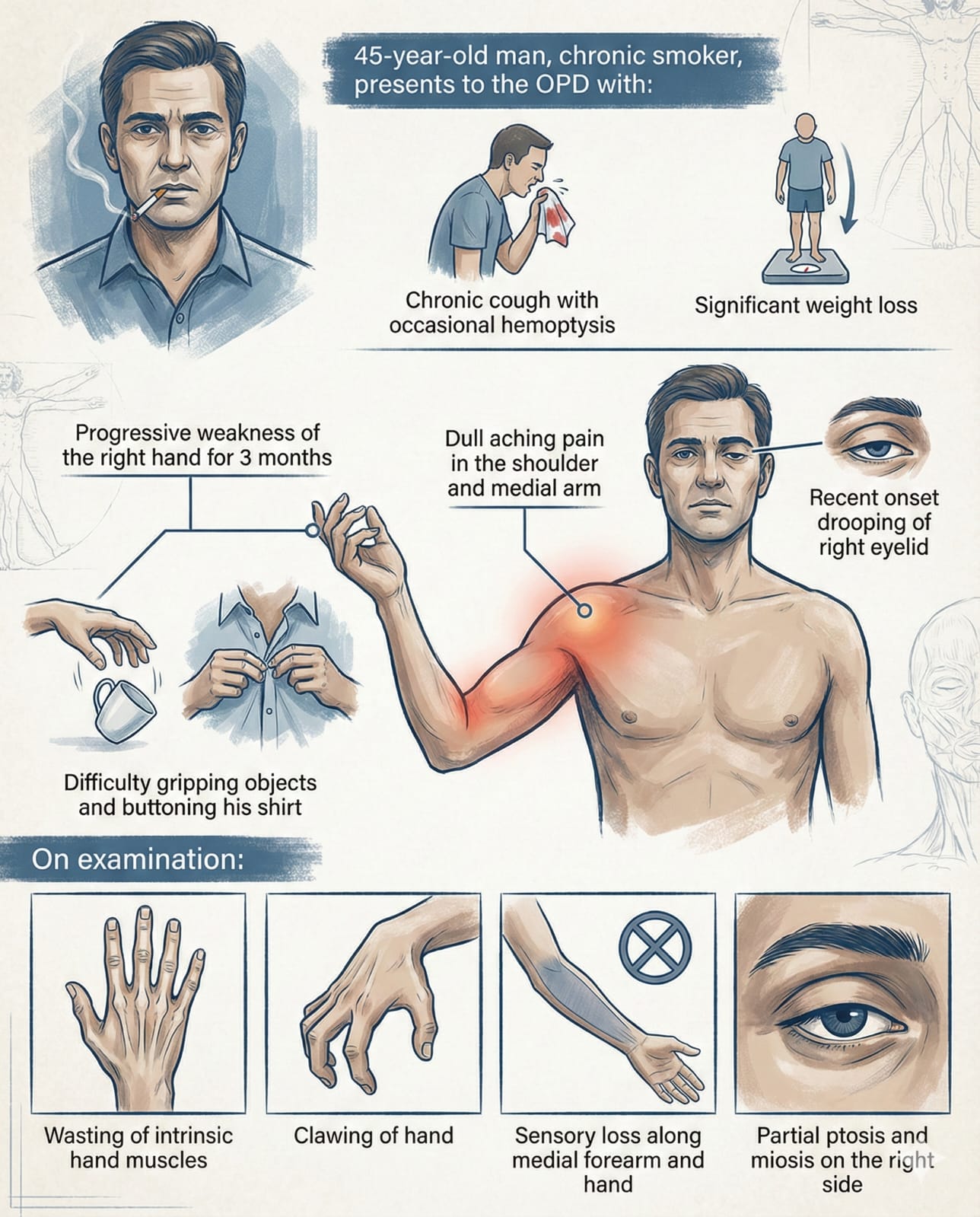
- 🌄 Pancoast tumour (superior sulcus tumour) = apical lung cancer with local invasion.
- Most linked to NSCLC (squamous cell, adenocarcinoma).
- Classically presents with ipsilateral Horner’s syndrome + severe shoulder pain.
🧠 Key Structures Invaded
- 🫁 Lung Apex → starting point.
- 💪 Brachial Plexus (C8–T1) → arm/hand pain, weakness, wasting.
- 👁️ Sympathetic Chain → Horner’s syndrome: ptosis, miosis, anhidrosis, enophthalmos.
- 🦴 Chest Wall / Ribs / Vertebrae → pain + destruction.
- 🗣️ Recurrent Laryngeal Nerve → hoarseness, “bovine cough.”
👩⚕️ Clinical Features
- 🎯 Shoulder pain → often misdiagnosed as MSK issue.
- 💨 Cough, haemoptysis, weight loss.
- 👁️ Horner’s syndrome (triad: ptosis, miosis, anhidrosis ± enophthalmos).
- 🗣️ Hoarseness / weak cough (recurrent laryngeal nerve).
- 🖐️ Systemic signs: digital clubbing, cachexia, nicotine stains, metastatic features.
📸 Example: Left Pancoast Tumour + Horner’s Syndrome
Ptosis often mild, but miosis + anhidrosis usually evident.

🔎 Investigations
- 📷 CXR: apical opacity, subtle → scrutinise carefully.
- 🧪 U&E: check for SIADH / hyponatraemia (ectopic ADH).
- 🦴 Bone profile: hypercalcaemia = mets/paraneoplastic.
- 🧪 LFTs: raised ALP = liver/bone involvement.
- 🖥️ CT chest: staging + invasion extent.
- 🔬 Biopsy: via bronchoscopy or CT-guided.
- 🧫 Sputum cytology: less sensitive but may show malignant cells.
🩺 Management
- 🩹 Pain & Palliation: opioids, nerve blocks, radiotherapy for pain control.
- ☢️ Radiotherapy: shrink tumour, symptom relief.
- 💉 Chemotherapy: systemic control (esp. NSCLC subtypes).
- 🔪 Surgery: rare (due to invasion); some centres attempt combined surgery + RT if limited spread.
- 🤝 MDT care: oncology, respiratory, radiology, palliative care.
📊 Prognosis
- ⚠️ Often late presentation → poor outcomes.
- 📈 5-yr survival ~20–30% if unresectable; better with trimodal therapy (chemo + RT + surgery in select cases).
- Improving survival with modern chemo-radiotherapy + immunotherapy.
📌 Exam Pearls
- 🎯 Shoulder pain + Horner’s = Pancoast until proven otherwise.
- 🧠 Don’t forget: recurrent laryngeal nerve → hoarseness.
- ⚠️ Apical lung lesions → scrutinise CXR apex carefully.
- 🔎 Paraneoplastic syndromes (SIADH, hypercalcaemia) may coexist.