Radicular syndromes
Radicular syndromes (radiculopathies) occur when a spinal nerve root is compressed, irritated, or inflamed 🦴💥.
This leads to pain, numbness, weakness, or motor dysfunction along the path of the affected nerve.
Symptoms follow dermatomal patterns and help localize the lesion.
📖 Definition
A radiculopathy = pain + neurological deficit (sensory, motor, or reflex) due to nerve root involvement.
It can affect the cervical, thoracic, or lumbar spine. Classic example = sciatica 🦵.
🩺 Common Causes
- 💥 Disc Herniation: Most common; nucleus pulposus compresses adjacent root.
- ⏳ Degenerative Disc Disease: Ageing ➝ foraminal narrowing.
- 📉 Spinal Stenosis: Central or foraminal narrowing compresses multiple roots.
- 🦴 Osteophytes: Bony spurs from osteoarthritis.
- 🤕 Trauma: Vertebral fracture or subluxation.
- 🦠 Infections / Tumours: Rare; e.g. spinal TB (Pott’s disease) or metastases.
🔎 Types of Radiculopathy
- 🧠 Cervical Radiculopathy: Radiating pain/numbness in arms & hands (C5–C8).
- 🦴 Thoracic Radiculopathy: Band-like pain around chest/abdomen ➝ can mimic angina or gallstones.
- 🦵 Lumbar Radiculopathy (Sciatica): Pain down buttock, thigh, calf ➝ most common (L4, L5, S1 roots).
📌 Symptoms
- ⚡ Pain: Sharp, shooting, burning along dermatome.
- 🧊 Numbness/Tingling: “Pins & needles” in root distribution.
- 💪 Weakness: Specific to muscles supplied by the root.
- 🔨 Reflex Loss: Biceps, triceps, patellar, or Achilles reflex may be reduced.
- 🚶 Gait/Balance Problems: Especially in lumbar radiculopathy.
- Red Flags 🚩: Saddle anaesthesia, bilateral leg weakness, urinary retention → consider cauda equina syndrome (surgical emergency).
🧪 Diagnosis
- History: Pain distribution, onset, aggravating/relieving factors.
- Examination: Sensory testing, myotomes, reflexes ➝ helps localize root.
- Special Tests: Spurling’s test (cervical), Straight-leg raise (lumbar).
- Imaging:
- MRI 🥇: Gold standard for discs/stenosis.
- CT: Bony causes (osteophytes, trauma).
- X-ray: Alignment, spondylolisthesis.
- Nerve Studies: EMG/NCS confirm site/severity, distinguish from peripheral neuropathy.
💊 Treatment
- Conservative:
- 🏃 Physiotherapy: Core strengthening, posture correction.
- 💊 Medications: NSAIDs, neuropathic agents (gabapentin, pregabalin).
- 💉 Epidural Steroids: Reduce inflammation.
- Surgical (for severe/progressive cases):
- 🩻 Discectomy
- 🔩 Laminectomy
- 🛠️ Foraminotomy
📊 Prognosis
Most patients improve with conservative therapy within 6–12 weeks.
Surgery reserved for intractable pain or neurological deficit.
Chronic cases risk persistent neuropathic pain.
🛡️ Prevention
- 🪑 Good posture and ergonomic workspace.
- 🏋️ Core and back strengthening exercises.
- 📦 Proper lifting techniques; avoid heavy strain.
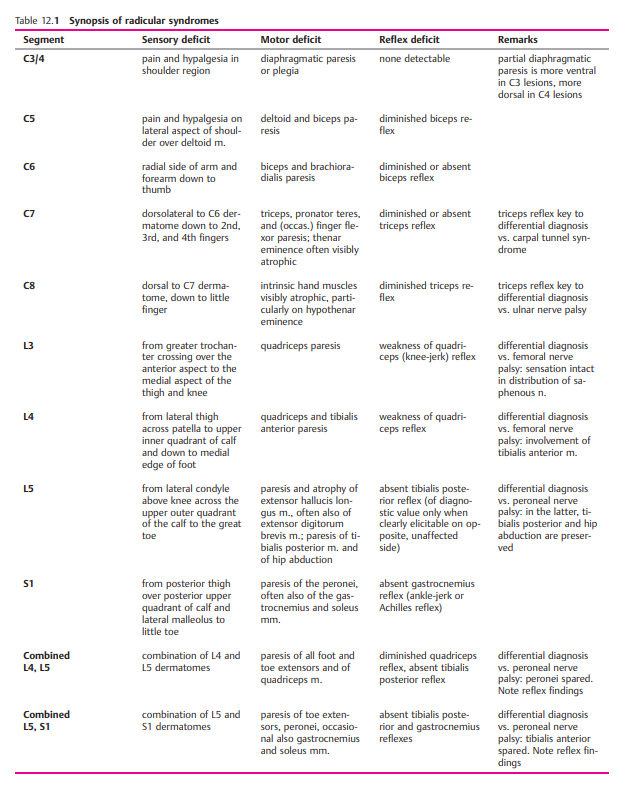
🧩 Cervical Nerve Root Syndromes
| Nerve Root | Pain | Sensory Loss | Weakness | Reflex |
|---|
| C5 | Neck → shoulder | Lateral upper arm | Deltoid, supraspinatus | ↓ Biceps |
| C6 | Neck → thumb | Lateral forearm, thumb | Biceps, wrist extensors | ↓ Biceps & brachioradialis |
| C7 | Neck → middle finger | Posterior forearm, middle finger | Triceps, wrist flexors | ↓ Triceps |
| C8 | Neck → little finger | Medial forearm, ring/little finger | Finger flexors, hand intrinsics | - |
🦵 Lumbar Radiculopathy (Sciatica)
| Nerve Root | Pain | Sensory Loss | Weakness | Reflex |
|---|
| L3 | Back → anterior thigh | Anterior thigh | Hip flexion, knee extension | ↓ Patellar |
| L4 | Back → medial shin | Medial thigh/shin | Knee extension, dorsiflexion | ↓ Patellar |
| L5 | Back → top of foot | Lateral calf, dorsum of foot | Dorsiflexion, big toe extension | - |
| S1 | Back → sole of foot | Lateral foot/sole | Plantarflexion | ↓ Achilles |