
🦴 Spinal Claudication vs Vascular Claudication: Spinal claudication often has neurological symptoms, worsens with spinal extension, improves with flexion (e.g. leaning forward on a shopping trolley 🛒), and pedal pulses are usually present. Classic symptoms: back, buttock, thigh, and calf pain provoked by walking/extension and relieved by flexed posture.
📖 About
- Spinal stenosis = narrowing of the spinal canal, nerve root canal, or intervertebral foramen.
- This narrowing → nerve root compression → ischaemia → pain in the back, buttock, or legs triggered by exercise or posture.
🔎 Aetiology
- Congenital: e.g. achondroplasia, idiopathic small canal.
- Acquired degenerative (common, age 50–70): due to facet joint hypertrophy, disc bulging, and thickened ligamentum flavum.
🔗 Associations
- Congenital spinal stenosis (achondroplasia, idiopathic).
- Degenerative changes (disc & facet hypertrophy).
- Spondylolisthesis or spondylolysis.
- Iatrogenic (post-laminectomy narrowing).
- Metabolic/bony disorders (e.g. Paget’s disease).
🧑⚕️ Clinical Features
- More common in women than men.
- Symptoms:
- Back + buttock pain.
- Neurogenic claudication: leg pain when walking 🚶♂️, worse in extension, eased in flexion.
- Progressive leg numbness/weakness, falls.
- In severe cases: bladder/bowel involvement (red flag for urgent review ⚠️).
🧪 Investigations
- MRI 🥇: gold standard, assesses stenosis, nerve roots, and soft tissue detail.
- CT 🖼️: good for bony detail (less soft-tissue resolution).
- CT myelography: adds contrast outlining canal if MRI not possible/contraindicated.
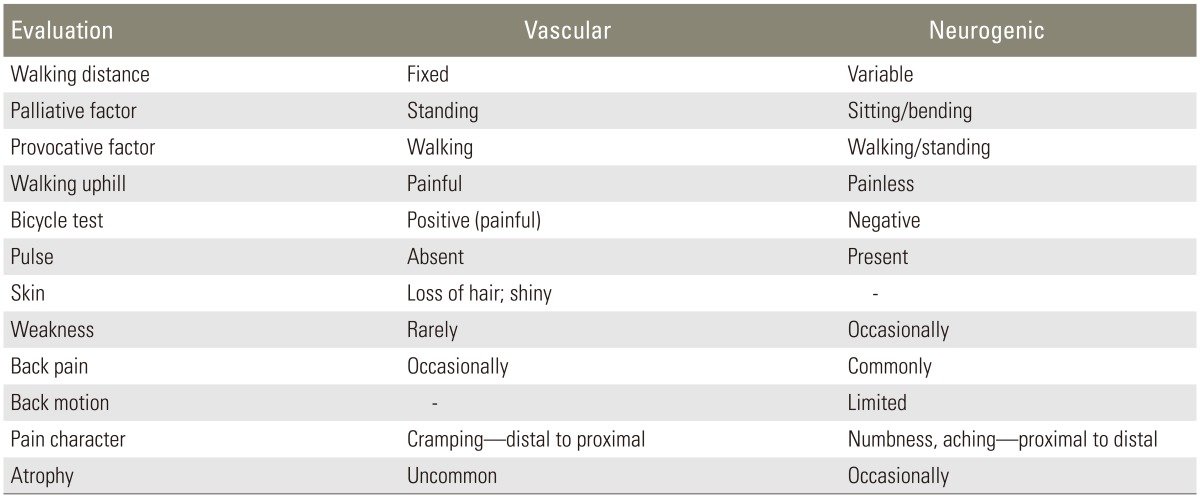
⚖️ Differential Diagnosis
- Vascular claudication (ABI testing, pulses absent/weak).
- Hip osteoarthritis or other joint disease.
- Peripheral neuropathy (diabetes, B12 deficiency).
- Combination of vascular + spinal disease can occur in older patients.
✅ Surgical decompression with preservation of facet joints can relieve symptoms effectively when conservative treatment fails.
🩺 Management
- Conservative (often first-line):
- Analgesia: paracetamol/NSAIDs for pain relief.
- Activity modification + supervised exercise 🏃 to improve function.
- Epidural steroid injections: temporary relief in selected cases.
- Surgical:
- Decompression (laminectomy ± fusion if instability).
- Considered if symptoms persist/worsen or neurological deficits develop.
- Up to one-third of patients deteriorate without surgery 📉.