
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Diabetes Mellitus Type 2 ✅
Related Subjects: |Diabetes Mellitus: Basics |Type 1 Diabetes Mellitus | Type 2 Diabetes Mellitus | Type 3c Diabetes Mellitus |Gestational Diabetes |HbA1c |Hyperglycaemic Hyperosmolar State (HHS) |Diabetic Nephropathy |Diabetic Retinopathy |Diabetic Neuropathy |Diabetic Amyotrophy |Maturity Onset Diabetes of the Young (MODY) |Diabetes: Complications |Hypoglycaemia |Diabetic Ketoacidosis (DKA) Adults |Alcoholic Ketoacidosis |Euglycaemic Ketoacidosis (euDKA) with SGLT2 Inhibitors |Causes of Ketoacidosis
🧠 Type 2 diabetes (T2DM) is driven by insulin resistance (reduced cellular response to insulin) plus progressive beta-cell failure. Early disease is often “high insulin, high glucose”; later disease becomes “low insulin for the level of glucose”, which is why many people eventually need injectable therapy. Persistent hyperglycaemia damages blood vessels via glycation, oxidative stress and endothelial dysfunction → microvascular (eyes, kidneys, nerves) and macrovascular (MI, stroke, PAD) disease.
📖 Overview
- Who gets it? Strong association with age, central adiposity, family history, ethnicity, gestational diabetes history, PCOS, and cardiometabolic risk.
- What’s happening? Hepatic glucose output ↑, muscle glucose uptake ↓, adipose lipolysis ↑ → fatty acids worsen insulin resistance; islet amyloid may be seen in longstanding disease.
- Key point: Many people are asymptomatic for years - so diagnosis often follows opportunistic testing or complication screening.
⚠️ Diagnosis (adults)
- HbA1c ≥ 48 mmol/mol (6.5%) (repeat/confirm if asymptomatic; avoid HbA1c if factors make it unreliable: haemoglobinopathies, recent transfusion, haemolysis, advanced CKD etc.).
- Fasting plasma glucose ≥ 7.0 mmol/L (repeat if asymptomatic).
- Random plasma glucose ≥ 11.1 mmol/L + symptoms (polyuria, polydipsia, weight loss).
- OGTT: 2-hour glucose ≥ 11.1 mmol/L (useful when diagnosis unclear or for “borderline” cases).
🩺 Clinical features
- Polyuria 🚽, polydipsia 💧, fatigue 😴, blurred vision 👁️.
- Recurrent infections (candida, UTIs), poor wound healing 🩹.
- Often presents with complications: neuropathy 🦶, CKD 🩺, retinopathy 👀, CVD ❤️🧠.
🔎 Baseline assessment at diagnosis (do early)
- CV risk: BP, smoking status, BMI/waist, lipids, QRISK3 discussion.
- Bloods: HbA1c, U&E/creatinine/eGFR, LFTs, lipids, FBC (anaemia affects HbA1c interpretation), B12 if on metformin long-term (baseline or later if symptomatic).
- Kidney: urine ACR + dip (albuminuria drives ACEi/ARB decisions and CKD staging).
- Complications screening: foot risk assessment + pulses/sensation; refer/ensure NHS diabetic eye screening.
- Think alternative diagnoses if atypical: very rapid onset, ketosis, low BMI, strong autoimmune history (consider LADA/T1), strong family pattern (consider MODY).
🎯 NICE targets & monitoring
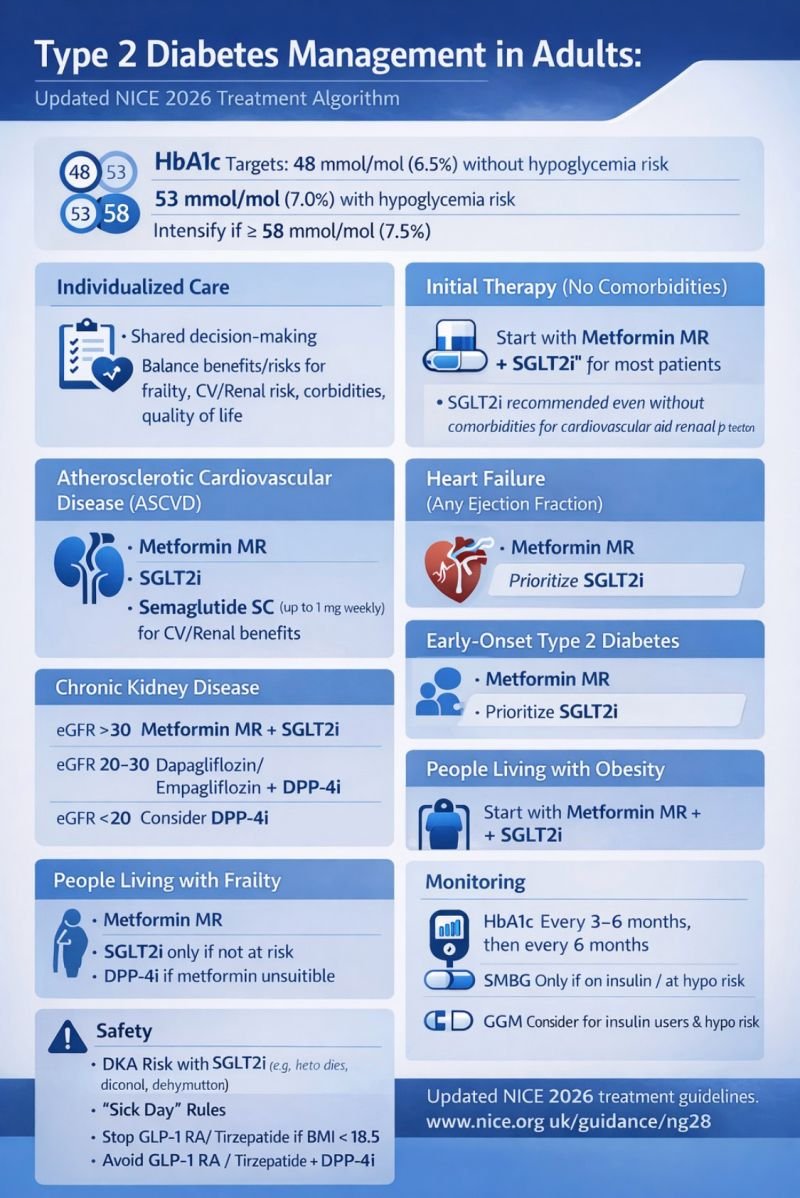
- HbA1c target (typical):
- 48 mmol/mol (6.5%) if managed by lifestyle alone or drugs not associated with hypoglycaemia.
- 53 mmol/mol (7.0%) if using drugs associated with hypoglycaemia (e.g., sulfonylureas, insulin).
- Consider relaxing targets (and simplifying regimens) for frailty, multimorbidity, recurrent hypos, limited life expectancy.
- Check HbA1c: every 3–6 months until stable, then at least 6-monthly.
🛠️ Management (stepwise, NICE-aligned)
✅ Core principle: choose glucose-lowering therapy based on cardiovascular disease, heart failure, CKD/eGFR, weight, and hypoglycaemia risk - not HbA1c alone. NICE updated NG28 in February 2026 with broader first-line use of SGLT2 inhibitors in several groups (including when metformin cannot be used).
Lifestyle (for everyone)
- Weight loss strategy (dietary pattern that the person can sustain), physical activity, sleep, alcohol moderation, smoking cessation 🚭.
- Offer structured education and support (and address health literacy + access to healthy food/exercise).
💊 Current NICE NG28 (Feb 2026) “which to start when” – quick list
- General rules (everyone): start medicines sequentially (not all at once), review HbA1c and tolerability before stepping up; pick agents based on ASCVD/HF/CKD, weight, and hypo risk.
- Most adults with T2DM (no specific high-risk group): start modified-release metformin. If metformin not tolerated/contraindicated → consider SGLT2 inhibitor monotherapy.
- Established atherosclerotic CVD (prior MI/stroke/PAD): start modified-release metformin + SGLT2 inhibitor + s/c semaglutide (Ozempic) up to 1 mg weekly (sequentially). If metformin can’t be used → SGLT2 inhibitor + s/c semaglutide.
- Heart failure (any EF): start modified-release metformin + SGLT2 inhibitor. If metformin can’t be used → SGLT2 inhibitor monotherapy.
- CKD:
- eGFR >30: modified-release metformin + SGLT2 inhibitor (or SGLT2 alone if metformin not tolerated).
- eGFR 20–30: dapagliflozin or empagliflozin + a DPP-4 inhibitor.
- eGFR <20: consider a DPP-4 inhibitor; if not suitable/effective → consider pioglitazone or insulin-based treatment.
- Early-onset T2DM (diagnosis <40 years): start modified-release metformin + SGLT2 inhibitor, and consider adding either a GLP-1RA (cardio-renal + glycaemic benefits) or tirzepatide (glycaemic benefits). If metformin can’t be used → SGLT2 inhibitor then consider GLP-1RA or tirzepatide.
- Living with obesity: start modified-release metformin + SGLT2 inhibitor. If metformin can’t be used → SGLT2 inhibitor monotherapy.
- Frailty: start with modified-release metformin and prioritise avoiding hypos (generally avoid sulfonylureas/complex insulin unless clearly needed).
Practical drug notes (quick safety): common T2DM drugs – doses + prescribing comments + side effects
- Metformin (IR/MR)
- Dose: start 500 mg once daily with food → increase every 1–2 weeks; common maintenance 1–2 g/day (IR split; MR often OD). Typical max 2 g/day.
- Prescribing: MR + slow titration reduces GI intolerance. Consider B12 deficiency in long-term use. Hold temporarily in significant acute illness/dehydration (“sick day”).
- Side effects: GI upset/diarrhoea, metallic taste; rare lactic acidosis risk in severe renal/hepatic failure or hypoxic states.
- Dapagliflozin (SGLT2 inhibitor)
- Dose: 10 mg once daily.
- Prescribing: Give clear sick-day rules (stop during acute illness, fasting, major surgery). Caution with diuretics/frailty (volume depletion). Check local eGFR criteria.
- Side effects: genital thrush, UTIs, dehydration/postural dizziness; rare euglycaemic DKA (think if nausea, abdominal pain, breathlessness even with normal-ish glucose).
- Empagliflozin (SGLT2 inhibitor)
- Dose: start 10 mg once daily; may increase to 25 mg once daily if appropriate (renal criteria apply).
- Prescribing: Same sick-day rules as above; consider cardio-renal benefit in HF/CKD groups per NG28.
- Side effects: as SGLT2 class-genital infections, volume depletion; rare DKA.
- Gliclazide (sulfonylurea)
- Dose: start 40–80 mg once daily with breakfast; titrate to response; max 320 mg/day (often split BD at higher doses).
- Prescribing: Useful when you need quicker HbA1c drop or if cost is key, but avoid in those at high hypo risk (frail, CKD, irregular meals). Provide driving/hypo education.
- Side effects: hypoglycaemia, weight gain; can be prolonged in renal impairment.
- Pioglitazone (TZD)
- Dose: 15–30 mg once daily → max 45 mg once daily.
- Prescribing: Takes weeks to work; avoid in heart failure or significant oedema. Consider fracture risk and avoid if bladder cancer history/unexplained haematuria.
- Side effects: oedema, weight gain, heart failure exacerbation, fractures (esp. women), rare hepatic issues.
- Sitagliptin (DPP-4 inhibitor)
- Dose: 100 mg once daily; commonly renal-adjust to 50 mg OD (moderate impairment) or 25 mg OD (severe).
- Prescribing: Weight-neutral, low hypo risk; a useful “safe add-on” when other agents unsuitable. Remember renal dosing.
- Side effects: generally mild (URTI symptoms, headache); rare pancreatitis.
- Linagliptin (DPP-4 inhibitor)
- Dose: 5 mg once daily (often no renal adjustment).
- Prescribing: Handy in CKD where dosing simplicity matters; still review efficacy at follow-up.
- Side effects: as DPP-4 class; rare pancreatitis.
- Semaglutide (GLP-1 receptor agonist, s/c weekly)
- Dose: 0.25 mg weekly x 4 weeks → 0.5 mg weekly; if needed step up to 1 mg, then 2 mg weekly (in ≥4-week steps).
- Prescribing: Best for weight + glycaemic benefit; go slow to limit nausea. Reduce SU/insulin doses if combining to avoid hypos.
- Side effects: nausea, vomiting, diarrhoea/constipation, reflux; gallbladder disease; rare pancreatitis.
- Liraglutide (GLP-1 receptor agonist, s/c daily)
- Dose: 0.6 mg daily for ≥1 week → 1.2 mg daily; if needed 1.8 mg daily.
- Prescribing: Daily alternative where weekly not preferred; titrate slowly for tolerability.
- Side effects: GI upset (esp. early), gallbladder disease; rare pancreatitis.
- Tirzepatide (dual GIP/GLP-1, s/c weekly)
- Dose: 2.5 mg weekly x 4 weeks → 5 mg weekly; then ↑ by 2.5 mg every ≥4 weeks to max 15 mg weekly.
- Prescribing: Very effective for HbA1c and weight; GI-limited titration. Review concomitant SU/insulin to reduce hypo risk.
- Side effects: nausea/vomiting, diarrhoea/constipation, reduced appetite; gallbladder disease; rare pancreatitis.
- Basal insulin (e.g., glargine/degludec/detemir)
- Dose: common start 10 units once daily (or ~0.1–0.2 units/kg/day). Titrate e.g. +2 units every 3 days to fasting target while avoiding hypos.
- Prescribing: Continue metformin if tolerated; consider stopping/reducing sulfonylurea if hypos. Teach injection technique, hypo management, SMBG, and sick-day rules.
- Side effects: hypoglycaemia, weight gain; lipohypertrophy if poor site rotation.
💉 When to Start Insulin (Type 2 Diabetes) – concise
Start insulin if: symptomatic hyperglycaemia, persistent HbA1c above target despite optimised therapy, catabolic features/weight loss (± ketones), acute illness/steroids/surgery with severe hyperglycaemia, or when other agents are unsuitable (e.g., advanced CKD/intolerance). How to start: usually basal insulin (long-acting) and titrate to fasting glucose; consider GLP-1RA + basal to limit weight gain and insulin dose.
| Reason | Clues | Why insulin | Notes |
|---|---|---|---|
| Symptomatic hyperglycaemia | Polyuria/polydipsia, infections, blurred vision; very high CBG | Rapid symptom relief + reverses glucotoxicity | Start basal; review other meds; sick-day rules |
| HbA1c remains high | Above individual target despite adherence + escalation | Progressive beta-cell failure | Check adherence/technique and secondary causes first |
| Catabolic state / possible insulin deficiency | Weight loss, dehydration, ketones | Stops lipolysis/proteolysis; prevents ketosis | Consider LADA/T1; don’t miss DKA/HHS |
| Acute stress hyperglycaemia | Sepsis, MI/stroke, peri-op, high-dose steroids | Most controllable therapy during stress | Often temporary; follow inpatient protocols |
| Limited medication options | Intolerance/contraindications; advanced CKD | Works when other agents unsuitable | Lower doses in CKD; higher hypo risk |
| Recurrent severe hyperglycaemia | HHS or repeated admissions | Reduces recurrence risk | Needs close follow-up/education |
| Pregnancy planning / pregnancy | Pre-existing T2DM needing tighter control | Preferred/most reliable glucose control | Specialist pathway |
| Preference / regimen simplification | Tablet burden, side-effects, QoL issues | Basal insulin can simplify control | Shared decision-making; driving/hypo education |
🩺 Cardiovascular risk reduction (UK context)
- Blood pressure targets (commonly used with diabetes): aim <140/80 mmHg, or <130/80 mmHg if kidney, eye or cerebrovascular damage; use ACEi/ARB particularly if albuminuria.
- Statins: primary prevention typically atorvastatin 20 mg nightly when QRISK3 ≥10% (and consider even if <10% if risk may be underestimated or patient preference).
- Antiplatelet: not routine primary prevention; use for established ASCVD per cardiology guidance.
👵 Older adults / frailty
- Prioritise avoiding hypoglycaemia, falls, and medication burden; simplify regimens.
- Consider relaxing HbA1c targets and deprescribing sulfonylureas/complex insulin if hypos or limited benefit.
📚 References (NICE / UK)
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery