
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Tonsilitis
Related Subjects: |Assessing Hearing Loss |Benign Paroxysmal Positional Vertigo (BPPV) |Cholesteatoma |Epistaxis (Nosebleeds) |Acute Mastoiditis |Nasal polyps |Acute Sinusitis |Sudden Sensorineural Hearing loss (SNHL) |Causes of Vertigo
👩⚕️ Tonsillitis = acute infection of the palatine tonsils, usually viral but sometimes bacterial. Most children experience it; adults less often, but complications (e.g. quinsy) are more severe. Always consider red flags → stridor, drooling, severe dysphagia → 🚨 emergency referral.
🦠 Aetiology
- Viral: EBV (infectious mononucleosis), HSV, Adenovirus 🤒
- Bacterial: Group A β-haemolytic Streptococcus (Strep pyogenes), Mycoplasma, Corynebacterium diphtheriae
🧾 Clinical Presentation
- Severe sore throat, fever 🌡️, headache, malaise
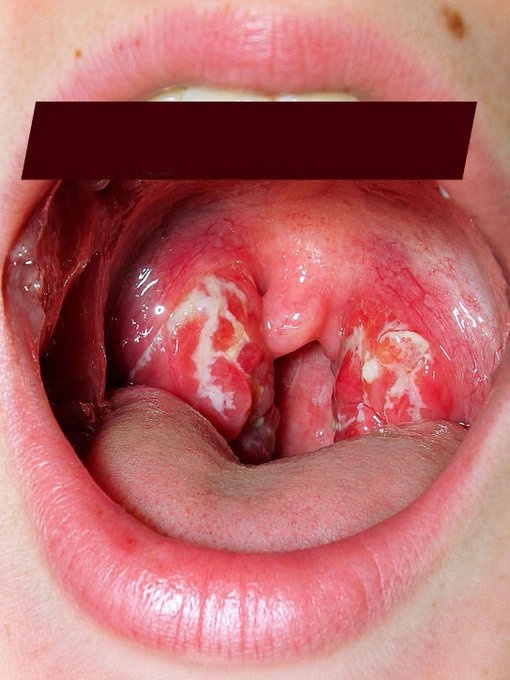
- Tonsillar findings: erythema, exudates, enlargement (torch often needed)
- Lymph nodes: tender anterior cervical lymphadenopathy
- Viral → coryzal symptoms; EBV → splenomegaly + marked fatigue
- Bacterial → white tonsillar exudate more likely
📊 Paradise Criteria (for “true” tonsillitis episodes)
Sore throat + ≥1 of:
- Fever >38.3°C 🌡️
- Swollen/tender cervical lymph node >2 cm
- Tonsillar exudate
- Positive strep culture
👶 Tonsillitis in Children
- Frequent, but tends to improve with age
- Significant impact on schooling (3–5 days absence/episode)
🧑 Tonsillitis in Adults
- Less common than children, but usually more severe
- Can cause prolonged work absence
- Complication: Peritonsillar abscess (Quinsy) → trismus, muffled “hot potato” voice, uvula deviation 🚨
🚨 Red Flags (do not attempt throat exam)
- Stridor, drooling, severe respiratory distress
- Very unwell/systemic sepsis
- Dysphagia, muffled voice, suspicion of epiglottitis
- Immediate hospital transfer required 🚑
🔍 Investigations
- FBC, CRP, U&E in unwell patients
- Throat swab for bacterial culture
- EBV serology (Monospot/Paul Bunnell), atypical lymphocytosis on FBC
⚠️ Complications
- Local: peritonsillar abscess (quinsy), retropharyngeal abscess
- Systemic: scarlet fever, rheumatic fever, glomerulonephritis
- EBV: hepatitis, prolonged fatigue, splenic rupture (rare)
🏥 Severe Complications
- Quinsy: fever, trismus, uvula deviation, “hot potato” voice → ENT referral + IV antibiotics, drainage
- Retropharyngeal abscess: neck swelling, stridor, sepsis → surgical emergency
- Lemierre’s syndrome: septic thrombophlebitis of jugular vein → ICU risk
📌 Admission Criteria
- Airway compromise (stridor, drooling, severe dysphagia)
- Severe systemic illness or dehydration
- Peritonsillar cellulitis/abscess
- Immunocompromised, diphtheria suspicion, or unusual systemic illness
💊 Management
- Analgesia: paracetamol/ibuprofen for fever & pain
- Hydration: oral fluids; IV if unable to swallow
- Antibiotics (if severe/systemic, bacterial suspected):
- First-line: Penicillin V (phenoxymethylpenicillin) 5–10 days
- Avoid amoxicillin in EBV → rash 🚫
- Alternative: clarithromycin if penicillin-allergic
- Tonsillectomy: Consider if recurrent tonsillitis (Paradise criteria) or after quinsy → ENT referral
Streptococcal Tonsilitis
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery