
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Acute Cholecystitis ✅
Related Subjects:Acute Cholecystitis |Acute Appendicitis |Chronic Peritonitis |Abdominal Aortic Aneurysm |Ectopic Pregnancy |Acute Cholangitis |Acute Abdominal Pain |Penetrating Abdominal Trauma |Acute Pancreatitis |Acute Diverticulitis
⚠️ Mortality: Acute calculous cholecystitis has <10% mortality with prompt hospital management. However, 🔥 Acute Acalculous Cholecystitis (more common in critically ill/ICU patients) carries a mortality up to 50% 🚨 and requires urgent recognition and intervention. 💡 Teaching Tip: Always distinguish calculous from acalculous; high mortality in ICU means early suspicion is lifesaving.
| 🩺 Initial Management Summary |
|---|
|
ℹ️ About
- 📊 Prevalence: Gallstones affect ~10% of the population; 10–20% symptomatic.
- 🧪 Pathophysiology: Cystic duct obstruction → ↑ intraluminal pressure → bile stasis → gallbladder wall inflammation. 💡 Tip: Remember Charcot’s triad for cholangitis differs from Murphy’s sign for cholecystitis.
- 👩 Demographics: More common in women; incidence rises with age (♀ 24%, ♂ 15% by 70 years).
- 🔪 Treatment: Symptomatic patients usually require laparoscopic cholecystectomy after CBD stones excluded.
🧪 Aetiology
- 💧 Lithogenic bile: ↑ cholesterol, ↓ bile salts → stone formation.
- 🚪 Cystic duct obstruction: Primary trigger → gallbladder inflammation.
- 🦠 Secondary infection: Often E. coli, Klebsiella, Enterococcus.
- ⚠️ Empyema: Pus-filled gallbladder → urgent surgery. 💡 Exam Tip: Empyema = sepsis risk; do not delay surgery for antibiotics alone.
⚠️ Risk Factors
- 👵 Age >50, 👩 Female, Caucasian
- 🍔 Obesity, rapid weight loss, diabetes, metabolic syndrome
- 🧬 Crohn’s (terminal ileum), cholestyramine therapy
- 🤰 Pregnancy, cystic fibrosis
💎 Types of Gallstones
| Type | Description | Incidence |
|---|---|---|
| ⚪ Mixed | Cholesterol + bile salts + calcium; most common. | 70% |
| 🟡 Cholesterol | Solitary; linked with hyperlipidaemia, pregnancy; “strawberry GB”. | 20% |
| ⚫ Pigment | Dark; associated with haemolysis (e.g., sickle cell). | 5% |
| 🟤 Brown | Linked to infection (Clonorchis); rare in UK. | Rare |
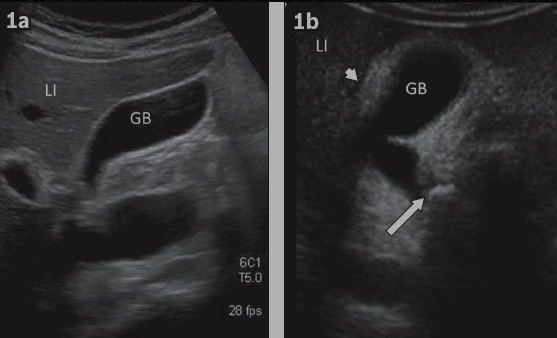
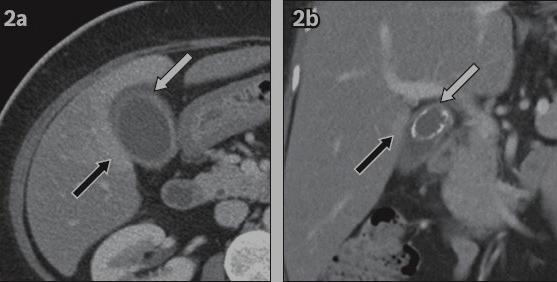
Cholecystitis Imaging (USS & CT)
Oblique coronal US: thickened GB wall, pericholecystic fluid, impacted calculus in GB neck. LI = liver.
CT axial/coronal: thickened GB wall, pericholecystic fat stranding (white arrow), reactive hyperaemia in adjacent liver (black arrow); large calculus visible.
🩺 Clinical Features
- ⚡ Sudden, severe RUQ pain → radiates to right shoulder/scapula
- 🤮 Nausea, vomiting, anorexia, fever
- 🖐️ Murphy’s sign: Inspiratory arrest on RUQ palpation
- 🟡 Jaundice → consider CBD stone/cholangitis 💡 Teaching Tip: Pain + Murphy’s sign is classic; jaundice suggests a different pathology or complication.
🔎 Investigations
- 🧪 Bloods: leukocytosis, ↑ CRP, mildly deranged LFTs; ↑ bilirubin if CBD involved
- 🖥️ USS: 1st-line → stones, wall thickening, pericholecystic fluid, sonographic Murphy’s sign
- 🩻 CT: complications (abscess, perforation)
- 💿 MRCP: best for CBD stones
- 🛠️ ERCP: diagnostic + therapeutic for CBD stones
📐 Calot’s Triangle: Cystic duct, common hepatic duct, cystic artery. Identify clearly to avoid bile duct injury during surgery. 💡 Exam Tip: Knowledge of anatomy reduces iatrogenic injury risk.
🚨 Complications
| Complication | Presentation | Management |
|---|---|---|
| 🧴 Gallbladder empyema | Persistent RUQ pain, high fever/rigors, sepsis | Sepsis 6 → IV fluids, blood cultures, antibiotics + urgent cholecystectomy/percutaneous cholecystostomy if high risk |
| 🦴 Gangrenous cholecystitis | Severe RUQ pain, systemic toxicity | Resuscitate, IV antibiotics, urgent cholecystectomy (senior input) |
| 💥 Emphysematous cholecystitis | Severe pain, sudden sepsis, often diabetics | Immediate resuscitation, IV antibiotics, urgent surgery/cholecystostomy |
| 🕳️ Perforation | Worsening pain, peritonism, sepsis | Sepsis management + urgent surgery; consider percutaneous drainage if localised |
| 🧫 Pericholecystic collection/abscess | Persistent RUQ pain/fever, palpable mass | IV antibiotics, image-guided drainage ± delayed cholecystectomy |
| 🟡 Choledocholithiasis | Jaundice, pale stools, dark urine, intermittent RUQ pain | Risk stratify (LFTs/USS/MRCP), ERCP extraction, cholecystectomy |
| 🚑 Ascending cholangitis | Charcot triad: fever, RUQ pain, jaundice; ± hypotension/confusion (Reynolds pentad) | Sepsis 6 + IV antibiotics, urgent biliary decompression (ERCP/PTC) |
| 🫀 Gallstone pancreatitis | Epigastric pain radiating to back, vomiting, ± jaundice | Supportive care, ERCP if cholangitis/obstruction, cholecystectomy during index admission if feasible |
| 🔒 Mirizzi syndrome | Obstructive jaundice ± RUQ pain | Specialist imaging, HPB input, definitive surgery |
| 🔁 Cholecystoenteric fistula / gallstone ileus | Older patient, SBO, vomiting/distension | Resuscitation, NG tube, urgent surgery: enterolithotomy ± staged fistula repair |
| 🎯 Gallbladder carcinoma | Persistent RUQ pain, weight loss, anorexia, jaundice | Urgent referral, CT staging, HPB MDT management |
🎭 Differentials
- Peptic ulcer disease, liver abscess
- Acute pancreatitis
- MI (atypical pain), pneumonia (referred pain)
💊 Management
- 💉 Analgesia (IV morphine/alternative), NBM
- 🧪 IV antibiotics (cefuroxime + metronidazole / local protocol)
- 🔪 Laparoscopic cholecystectomy = definitive treatment (ideally 24–72 h)
- ⏳ Delayed surgery (~6 weeks) if high-risk/unstable
- 🛠️ ERCP for CBD stones prior to surgery 💡 Teaching Tip: Definitive surgery is key; antibiotics alone are not curative.
👵 Frail / Elderly Patients
⚠️ Atypical Presentation: In frail or elderly patients, acute cholecystitis often presents without classic signs. Fever and Murphy’s sign may be absent, and confusion, lethargy, or reduced oral intake may be the main features. 💡 Teaching Tip: Always consider acute cholecystitis in frail patients with unexplained delirium or functional decline. 🩺 Management Considerations: Careful ABC assessment, IV fluids, analgesia, and IV antibiotics remain first-line.💡 Surgical decisions require MDT input (geriatrician + surgeon) considering comorbidities and physiological reserve and patient choice. Failure to settle conservatively then INR to place a percutaneous cholecystostomy is often preferred if operative risk is high, with delayed elective cholecystectomy once stabilized. Some very frail patients may not be fit for either.
📚 References
Case – Acute Cholecystitis
46-year-old woman presents with RUQ pain radiating to back, fever, nausea after fatty meal. Positive Murphy’s sign, raised WBC/CRP, mildly cholestatic LFTs. USS: gallstones, wall thickening, pericholecystic fluid. Managed with ABCDE, IV fluids, analgesia, NBM, IV antibiotics (co-amoxiclav or cefuroxime + metronidazole if penicillin allergy), and early laparoscopic cholecystectomy (24–72 h). Consider percutaneous cholecystostomy if unstable. Monitor for complications: empyema, gangrene/perforation, CBD stones. Differentials: biliary colic, ascending cholangitis, gallstone pancreatitis. 💡 Exam Tip: Always link clinical features, labs, imaging, and management when answering short-answer or OSCE questions.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery