🩸 Anaemia is a reduction in haemoglobin concentration below the normal range for age/sex/pregnancy status.
It is a sign, not a diagnosis, so the important clinical task is to identify the underlying cause.
A structured approach using MCV, the blood film, reticulocyte response, and targeted tests usually narrows the differential quickly.
🔍 Definition
- Adult men: Hb < 130 g/L (13 g/dL)
- Adult non-pregnant women: Hb < 120 g/L (12 g/dL)
- Pregnancy: anaemia is usually defined as Hb < 110 g/L (11 g/dL)
📖 About
- Anaemia causes reduced oxygen-carrying capacity of blood.
- Symptoms depend on severity, speed of onset, age, and cardiorespiratory reserve.
- Rapid blood loss may cause severe symptoms despite only modest early changes in Hb.
- Chronic anaemia may be surprisingly well tolerated until Hb is quite low.
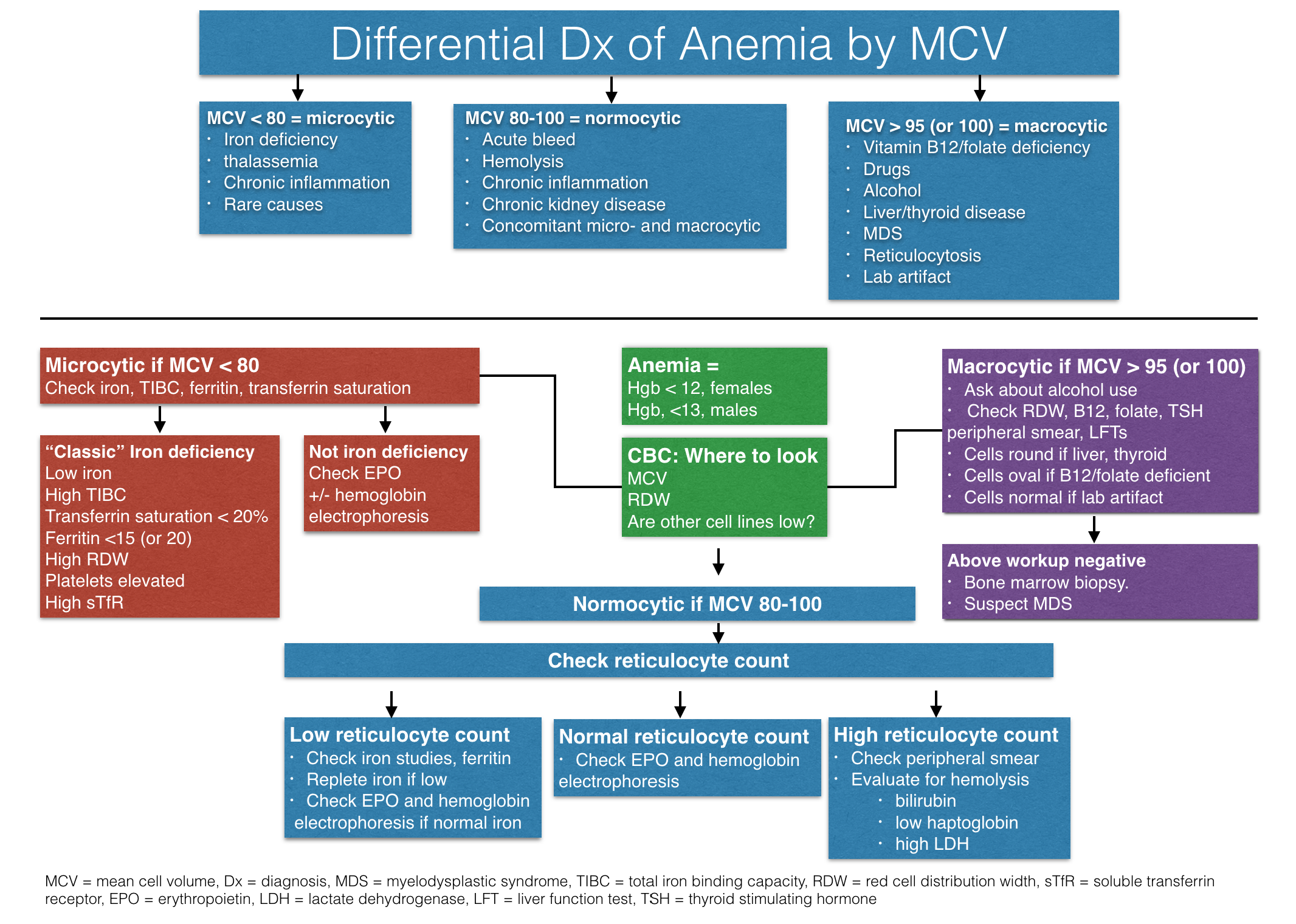
📊 Causes by MCV
- Microcytic (MCV < 80 fL): iron deficiency anaemia, thalassaemia, anaemia of chronic inflammation/disease, sideroblastic anaemia, lead toxicity.
- Normocytic (MCV 80–100 fL): acute blood loss, haemolysis, CKD, anaemia of chronic disease, marrow infiltration, endocrine disease, mixed deficiency states.
- Macrocytic (MCV > 100 fL): B12 deficiency, folate deficiency, alcohol excess, liver disease, hypothyroidism, reticulocytosis, myelodysplastic syndromes, drug effects.
📑 Classification of Anaemia
| Category |
Examples |
| Microcytic |
- Iron deficiency anaemia (IDA)
- Thalassaemia trait / thalassaemia syndromes
- Anaemia of chronic disease/inflammation
- Sideroblastic anaemia
- Lead poisoning
|
| Normocytic |
- Acute blood loss
- Haemolysis
- Chronic kidney disease
- Anaemia of chronic disease/inflammation
- Bone marrow infiltration / myelofibrosis
- Aplastic anaemia
- Endocrine disease (for example hypothyroidism, adrenal insufficiency)
|
| Macrocytic |
Megaloblastic
- Vitamin B12 deficiency
- Folate deficiency
Non-megaloblastic
- Alcohol excess
- Liver disease
- Hypothyroidism
- Reticulocytosis
- Myelodysplastic syndrome
- Drugs (for example hydroxycarbamide, methotrexate, azathioprine, antiretrovirals)
|
🩺 Clinical features
- Fatigue, lethargy, reduced exercise tolerance
- Pallor
- Exertional dyspnoea
- Palpitations
- Dizziness or presyncope
- Angina, syncope, or heart failure if severe or in people with cardiovascular disease
- Iron deficiency clues: pica, restless legs, glossitis, angular cheilitis, koilonychia
- B12 deficiency clues: peripheral neuropathy, gait disturbance, cognitive change, glossitis
- Haemolysis clues: jaundice, dark urine, splenomegaly
🧠 Initial clinical approach
- Confirm that anaemia is real and assess severity.
- Check whether it is isolated or associated with abnormal white cells or platelets.
- Use MCV as the first sorting tool, but do not stop there.
- Look at the reticulocyte count: low response suggests underproduction; high response suggests blood loss or haemolysis.
- Always ask about bleeding, GI symptoms, diet, alcohol, drugs, chronic disease, family history, and pregnancy status where relevant.
🧪 Core investigations
- FBC and blood film: Hb, MCV, MCH, RDW, platelet count, WCC, morphology
- Reticulocyte count
- Ferritin and iron studies
- Vitamin B12 and folate
- U&E / creatinine for CKD
- LFTs and TFTs if indicated
- CRP/ESR if inflammation/chronic disease suspected
- Haemolysis screen: bilirubin, LDH, haptoglobin, DAT if haemolysis suspected
- Coeliac serology in iron deficiency anaemia
- Hb electrophoresis if thalassaemia or haemoglobinopathy suspected
🔎 Iron deficiency anaemia (IDA)
- Ferritin is the most useful initial test; a low ferritin confirms iron deficiency.
- Ferritin is an acute-phase reactant, so a “normal” ferritin does not exclude iron deficiency if inflammation is present.
- In adults, especially men and postmenopausal women, always look for a cause of blood loss - particularly gastrointestinal loss.
- Screen all people with IDA for coeliac disease using coeliac serology.
- Consider menstrual loss, pregnancy, poor intake, malabsorption, NSAID use, and GI malignancy where appropriate.
🔎 Vitamin B12 and folate deficiency
- Vitamin B12 deficiency may be caused by pernicious anaemia, gastric surgery, ileal disease, metformin, vegan diet, or malabsorption.
- Folate deficiency may be caused by poor diet, alcohol excess, malabsorption, pregnancy, haemolysis, or drug therapy.
- Do not start folic acid alone until B12 deficiency has been excluded, because neurological injury from B12 deficiency may worsen or be masked.
- Check for intrinsic factor antibodies if pernicious anaemia is suspected.
🔎 Haemolytic anaemia
- Think of haemolysis if anaemia is accompanied by reticulocytosis, jaundice, raised LDH, low haptoglobin, or splenomegaly.
- Causes include autoimmune haemolysis, hereditary spherocytosis, G6PD deficiency, sickle cell disease, microangiopathy, infection, and drugs.
🔎 Anaemia in CKD
- CKD commonly causes a normocytic, normochromic anaemia due to reduced erythropoietin production.
- Iron deficiency should be identified and treated if present.
- ESA therapy should not be started in absolute iron deficiency without also managing the iron deficiency.
- Management often requires renal guidance if anaemia is persistent or advanced CKD is present.
💊 Management
- Treat the cause, not just the Hb result.
- Iron deficiency: oral iron is first-line in many patients; IV iron may be needed if oral iron is not tolerated, ineffective, or time is short before surgery.
- B12 deficiency: treat confirmed deficiency with hydroxocobalamin; lifelong treatment is needed in pernicious anaemia and many irreversible causes.
- Folate deficiency: oral folic acid after excluding or treating B12 deficiency.
- Thalassaemia trait: usually needs explanation and family counselling rather than iron, unless iron deficiency coexists.
- CKD: iron replacement and, if appropriate, erythropoiesis-stimulating agents under CKD guidance.
- Haemolysis / marrow failure / suspected malignancy: urgent specialist referral may be needed.
💉 Blood transfusion
- Transfusion is based on clinical status, not Hb alone.
- Consider urgency, symptoms, active bleeding, cardiovascular disease, and speed of onset.
- Severe symptomatic anaemia, haemodynamic compromise, or acute coronary symptoms need urgent assessment.
🚨 Red flags
- Pancytopenia or bicytopenia
- Suspected haemolysis
- Rapidly falling Hb
- Weight loss, night sweats, lymphadenopathy, hepatosplenomegaly
- Neurological features of B12 deficiency
- IDA in an adult man or postmenopausal woman without obvious explanation
- Severe anaemia with chest pain, syncope, heart failure, or haemodynamic instability
📚 References
💡 Clinical pearl:
Start with MCV + reticulocytes + ferritin + film.
Microcytic often means iron deficiency or thalassaemia.
Macrocytic means B12/folate, alcohol, liver, thyroid, marrow, or drugs.
Normocytic means think blood loss, haemolysis, CKD, chronic disease, or marrow pathology.
Always ask: Where is the blood loss? Is there haemolysis? Is the marrow responding?
