Conus Medullaris syndrome
Related Subjects:
|Transverse myelitis
|Acute Disseminated Encephalomyelitis
|Cervical spondylosis
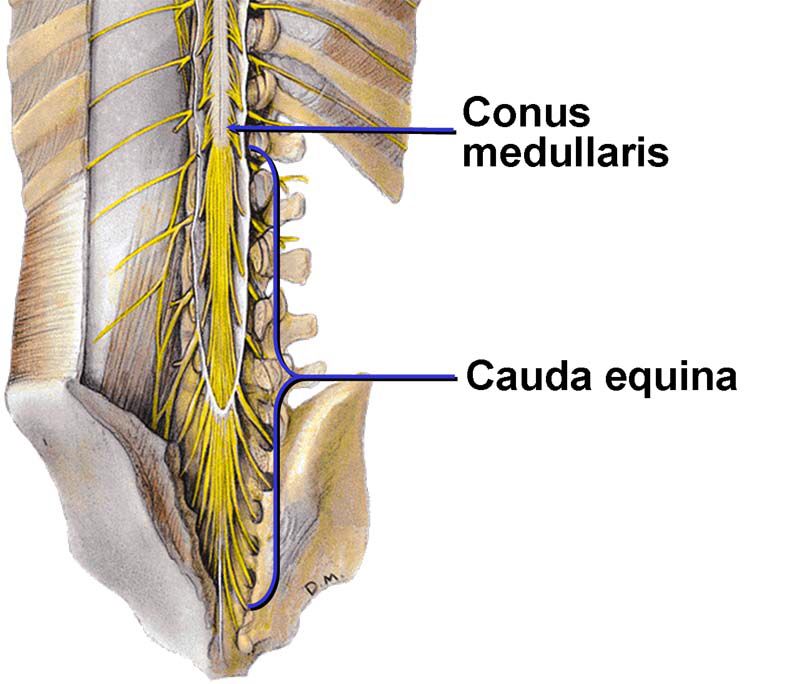
|Spinal Cord Anatomy
|Acute Disc Prolapse
|Spinal Cord Compression
|Spinal Cord Haematoma
|Foix-Alajouanine syndrome
|Cauda Equina
|Conus Medullaris syndrome
|Anterior Spinal Cord syndrome
|Central Spinal Cord syndrome
|Brown-Sequard Spinal Cord syndrome
|Internal Decapitation
🧠 About
- Conus Medullaris Syndrome is caused by a lesion at the L1 spinal level, affecting the tapered end of the spinal cord, the conus medullaris.
- It produces a mix of lower motor neuron (LMN) and upper motor neuron (UMN) signs, since both the spinal cord and the nerve roots can be involved.
⚠️ Aetiology
- Trauma – fractures or dislocations of the L1 vertebra.
- Malignancy – spinal tumours compressing the conus.
- Ischaemia – e.g. abdominal aortic aneurysm (AAA) rupture or infarction.
- Infections – epidural abscess, tuberculosis.
- Inflammatory and vascular causes – spinal cord infarction, vasculitis.
🩺 Clinical Features
- 📍 Sensory:
- “Saddle anaesthesia” – numbness/tingling in S3–S5 dermatomes (perineum, buttocks, inner thighs).
- Numb soles of feet (S2–S4 dermatomes).
- 💪 Motor:
- Mild, bilateral weakness in foot flexors (e.g. gastrocnemius).
- Lower limb motor function relatively preserved compared with sensory loss.
- Babinski sign may be positive (extensor plantar response).
- ⚡ Autonomic Dysfunction:
- Bladder – retention or overflow incontinence.
- Bowel – constipation or incontinence.
- Sexual dysfunction – e.g. erectile dysfunction in males.
- 🔁 Reflexes: Reduced/absent ankle reflexes (LMN involvement).
🔬 Investigations
- Bloods: FBC, U&E, ESR, calcium – rule out malignancy, infection, inflammation.
- MRI spine: Gold standard – lumbar + sacral levels to localise lesion.
CT myelography if MRI unavailable/contraindicated.
- Neurophysiology: EMG and nerve conduction studies – differentiate from other neuropathies.
- Urodynamics: Assess bladder dysfunction and autonomic impairment.
💊 Management
- Spinal Surgery: Urgent referral for decompression ± stabilisation.
- Surgical options: Laminectomy, decompression, tumour resection depending on cause.
- Antibiotics: IV antibiotics in infective cases (e.g. epidural abscess, TB).
- Rehabilitation: Multidisciplinary neurorehab – physiotherapy, occupational therapy, bladder & bowel training.
- Symptomatic:
- Pain relief (NSAIDs, analgesics).
- Bladder catheterisation ± bowel regimen to prevent complications.