
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Renal cell carcinoma ✅
Related Subjects: |Urothelial tumour s |Haematuria |Acute Urinary Retention |Anuria and Oliguria |Bladder cancer |Renal cell carcinoma |Benign Prostatic Hyperplasia |IgA nephropathy |Prostate Cancer |Henoch-Schonlein purpura |Glomerulonephritis
🔎 About Renal Cell Carcinoma (RCC)
- 🧬 Renal cell carcinoma (RCC) is the most common primary kidney cancer in adults, accounting for ~90% of renal malignancies.
- 👨🦳 Typically occurs in people aged 50–70 years and is around 2–3× more common in males.
- 🩺 Many cases are now detected incidentally on imaging performed for unrelated reasons.
- 📈 Incidence has increased with widespread use of abdominal CT and ultrasound.
🧬 Aetiology
- Genetic Syndromes
- 🧩 Von Hippel–Lindau (VHL) syndrome – mutation of the VHL tumour suppressor gene → predisposition to clear cell RCC.
- 🧬 Hereditary papillary RCC – autosomal dominant mutation affecting MET proto-oncogene.
- 🧬 Birt-Hogg-Dubé syndrome – folliculin gene mutation.
- 🧬 Hereditary leiomyomatosis and RCC – fumarate hydratase mutation.
- Lifestyle Factors
- 🚬 Smoking – strongest modifiable risk factor.
- ⚖️ Obesity – increased risk due to metabolic and hormonal effects.
- Medical Conditions
- 📈 Hypertension
- 🩺 Chronic kidney disease
- 🩸 Long-term dialysis and acquired cystic kidney disease
- Occupational Exposures
- 🏭 Heavy metals (e.g. cadmium)
- 🏭 Industrial solvents and dyes
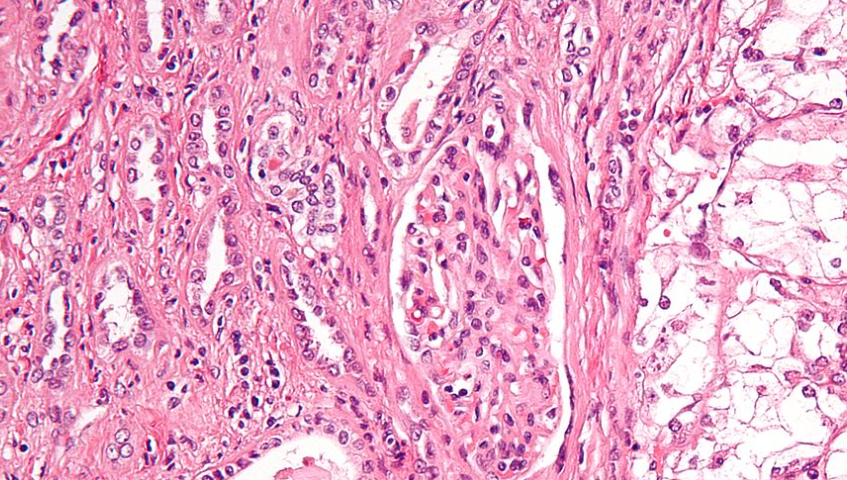
🧫 Histology
- RCC arises from the renal tubular epithelium.
- 📊 Major subtypes:
- Clear cell RCC (~75–80%) – most common and often associated with VHL mutation.
- Papillary RCC (~10–15%).
- Chromophobe RCC (~5%).
- 🧬 Tumours may invade renal veins and the inferior vena cava.
⚠️ Risk Factors
- 👨 Male sex
- 🚬 Smoking
- ⚖️ Obesity
- 📈 Hypertension
- 🩺 CKD and long-term dialysis
- 🧬 Genetic syndromes
- 🩸 Acquired cystic kidney disease
🩺 Clinical Features
- Classic triad (rare): 🩸 haematuria, flank pain, palpable abdominal mass.
- 📉 Constitutional symptoms: weight loss, fatigue, fever.
- 🍇 Left-sided varicocele (compression of left testicular vein).
- 🩸 Paraneoplastic syndromes:
- Polycythaemia (↑ erythropoietin)
- Hypercalcaemia (PTH-related peptide)
- Hypertension (renin secretion)
- Non-metastatic hepatic dysfunction (Stauffer syndrome)
- 🌍 Metastatic spread commonly to lungs, bones, liver, brain.
- 🫀 Tumour may extend into renal vein → inferior vena cava → right atrium.
🔍 Investigations
- 💉 Urinalysis: haematuria
- 📊 Blood tests: FBC, U&E, calcium, LFTs
- Imaging
- 🖥️ Ultrasound – may detect a renal mass.
- 🖼️ Contrast CT (renal protocol) – main diagnostic and staging investigation.
- 🧲 MRI – useful if venous invasion suspected or CT contraindicated.
- 🫁 CT chest for metastatic staging.
- 🧪 Renal tumour biopsy may be performed if systemic therapy is planned or diagnosis uncertain.
💡 Key concept: Many RCCs are now discovered incidentally on CT scans. Early-stage tumours are often asymptomatic and potentially curable with surgery.
🛠️ Management (UK Practice)
- General Measures
- 🚭 Smoking cessation
- ⚖️ Weight management
- 🩺 Optimisation of cardiovascular risk factors
- Surgical Treatment (Preferred for Localised Disease)
- 🔪 Partial nephrectomy – nephron-sparing surgery for small tumours (T1).
- ⚡ Radical nephrectomy – removal of kidney ± adrenal ± lymph nodes if larger or invasive tumour.
- Ablative Therapies
- 🔥 Radiofrequency ablation
- ❄️ Cryoablation
- Used for small tumours in patients unsuitable for surgery.
- Systemic Therapy (Metastatic Disease)
- 🛡️ Immune checkpoint inhibitors (e.g. nivolumab, pembrolizumab, ipilimumab)
- 🎯 Tyrosine kinase inhibitors (VEGF inhibitors) (e.g. sunitinib, pazopanib, cabozantinib)
- ⚡ Combination therapy often used first-line (e.g. immunotherapy + TKI).
- Radiotherapy
- 🎯 Primarily palliative for bone or brain metastases.
📊 Prognosis
- 📍 Localised disease → ~60–75% 5-year survival.
- 🌍 Metastatic disease → significantly lower survival.
- Outcome depends strongly on stage at diagnosis.
🩺 Case 1 – Localised RCC
A 58-year-old smoker presents with intermittent painless haematuria. CT scan shows a 5.2 cm enhancing upper-pole renal mass without metastases. Management: nephron-sparing partial nephrectomy. Post-operative follow-up includes surveillance CT imaging and renal function monitoring.
🩺 Case 2 – Metastatic RCC
A 72-year-old patient presents with weight loss, bone pain and hypercalcaemia. CT demonstrates an 8 cm renal mass with lung metastases. Management: systemic therapy with immune checkpoint inhibitor + VEGF-targeted therapy. Palliative radiotherapy may be used for symptomatic bone metastases.
📚 References
- NICE Kidney Cancer Guidance
- European Association of Urology (EAU) Guidelines
- American Cancer Society Kidney Cancer Resources
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery