
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Ulnar nerve
Related Subjects: |Radial Nerve |Median Nerve |Ulnar Nerve |Musculocutaneous nerve |Axillary nerve |Brachial plexus
✋ Although the 4th & 5th digits are held in the clawed position when the ulnar nerve is injured at the wrist, a high lesion (above elbow) paralyses the long flexors → loss of this sign. This is called the ulnar paradox 🧩.
🩻 Anatomy of the Ulnar Nerve
- Origin: medial cord of brachial plexus (C8, T1).
- Course:
- Descends medial arm → passes posterior to medial epicondyle (“funny bone”).
- Runs between flexor carpi ulnaris & FDP in forearm.
- Enters hand via Guyon’s canal near pisiform.
The ulnar nerve is a major nerve of the upper limb, originating from the brachial plexus (C8–T1). It supplies key forearm flexors and most intrinsic hand muscles, as well as sensation to the medial 1½ fingers.
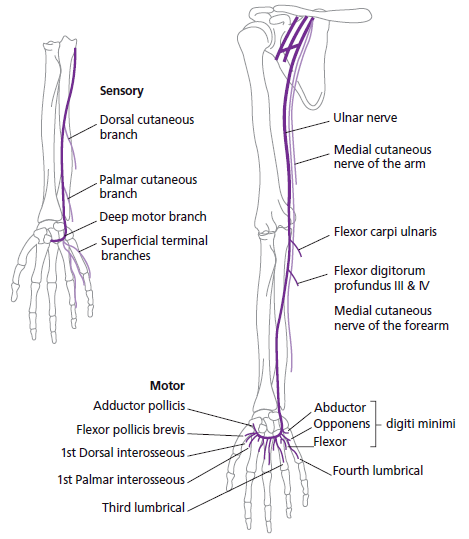
🌿 Branches
- Forearm muscular: flexor carpi ulnaris, medial half of FDP.
- Hand muscular: hypothenar muscles, interossei, medial 2 lumbricals, adductor pollicis.
- Sensory:
- Dorsal cutaneous branch → dorsum medial 1½ fingers.
- Palmar cutaneous branch → palmar medial 1½ fingers.
⚙️ Functions
- Motor: finger ab/adduction (interossei), grip & pinch strength, wrist flexion (FCU), DIP flexion of 4th & 5th (FDP).
- Sensory: medial hand + medial 1½ digits (palmar & dorsal).
🚨 Clinical Relevance
- Ulnar nerve entrapment:
- Elbow → cubital tunnel syndrome.
- Wrist → Guyon’s canal syndrome.
- Symptoms: paraesthesia in medial 1½ digits, weak grip, hand intrinsic wasting.
- Ulnar nerve injury:
- High lesion (elbow/humerus): FCU + FDP (digits 4–5) + intrinsic hand weakness → less obvious clawing (ulnar paradox).
- Low lesion (wrist): long flexors intact, intrinsic weakness → claw hand deformity of digits 4–5.
- Froment’s sign: thumb IP flexes (FPL via median nerve) when trying to pinch a paper due to weak adductor pollicis (ulnar).
- Claw hand deformity:
- Hyperextension of MCP + flexion of IP joints (digits 4–5).
- Caused by unopposed extensor digitorum + FDP action.
🧪 Investigations
- Clinical exam: interossei (finger ab/adduction), Froment’s sign, sensory testing.
- Nerve conduction studies / EMG.
- MRI/US if structural entrapment suspected.
💊 Management
- Conservative: activity modification, splints, physio, NSAIDs.
- Neuropathic pain management if required.
- Surgical decompression (cubital tunnel release, Guyon’s canal release) for persistent/severe cases.
📚 Summary
🔑 The ulnar nerve (C8–T1) supplies most intrinsic hand muscles and sensation to the medial 1½ digits. 👉 Low lesion → classic claw hand. 👉 High lesion → less clawing (ulnar paradox). 👉 Froment’s sign = key clinical test for adductor pollicis weakness.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery