Related Subjects:
|Antepartum haemorrhage
|Postpartum haemorrhage
|Acute Haemorrhage
|Placenta praevia
|Placenta abruption
⚠️ About
- Antepartum haemorrhage = any vaginal bleeding after 24 weeks gestation until delivery.
- Placental abruption = premature separation of the placenta from the uterine wall before birth.
- 🔑 It is a major cause of antepartum haemorrhage and a leading obstetric emergency.
- 🚨 Blood loss may be concealed (trapped behind placenta) → clinical severity can be underestimated.
📊 Aetiology
- Incidence ~1–2% of pregnancies.
- Bleeding occurs into the decidua basalis, shearing placenta away from uterus.
- Maternal uterine blood flow at term is 600–800 mL/min → risk of rapid, life-threatening haemorrhage.
⚠️ Risk Factors
- Pre-eclampsia / chronic hypertension
- Chorioamnionitis
- Cocaine use 🚬💉
- Polyhydramnios → sudden uterine decompression
- Trauma (RTC, falls, domestic violence)
- Smoking
- Male fetus
- Higher incidence in Black women
🩺 Clinical Features
- Vaginal bleeding (visible or concealed)
- Severe constant abdominal or back pain
- Uterus tense, tender, “woody” on palpation
- Uterine contractions or hypertonicity
- Fetal distress (abnormal CTG / absent FHR)
🔍 Differentials
- Placenta praevia
- Uterine rupture
- Appendicitis
- Chorioamnionitis
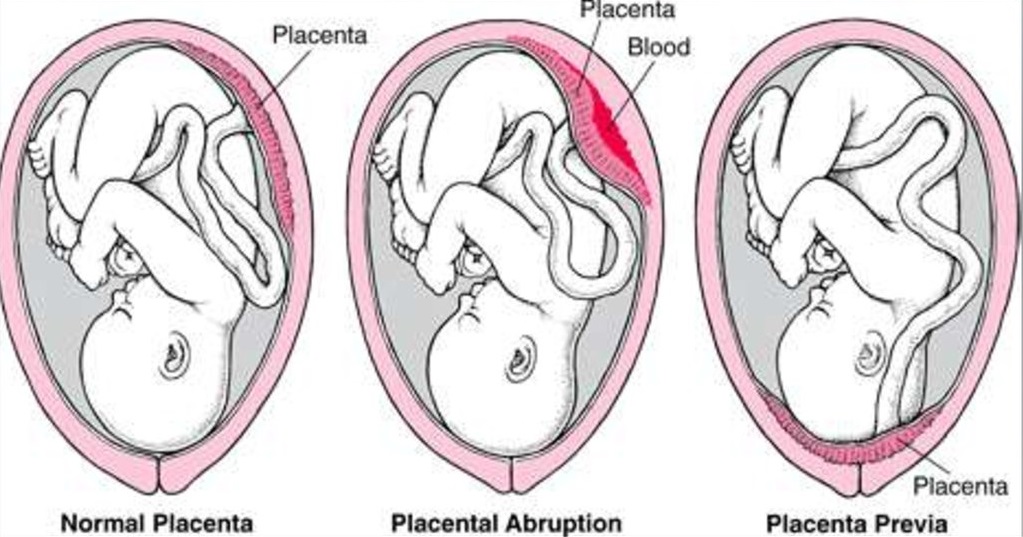
🖼️ Causes of Antepartum Haemorrhage
🧪 Investigations
- USS → poor sensitivity (only ~50% cases detected). Clinical diagnosis is key.
- Bloods: FBC, coagulation screen, fibrinogen (↓ early in DIC), U&E, cross-match 4–6 units.
- CTG for continuous fetal monitoring.
🏥 Management
- Stabilise mother first: large-bore IV access, IV fluids, cross-match, blood products as needed.
- Fetal viability: assess viability and CTG trace.
- Steroids: if preterm, give corticosteroids for lung maturity.
- Monitor for DIC: keep close watch on coagulation profile.
- Delivery:
- Vaginal delivery possible if mother/fetus stable.
- 🚨 Emergency C-section if heavy bleeding or fetal distress.
⚠️ Complications
- Maternal: haemorrhagic shock, DIC, ATN (renal injury), Couvelaire uterus (blood infiltration → uterine atony)
- Fetal: intrauterine death, prematurity, hypoxia
📌 Exam Pearls
- Visible PV loss ≠ severity → concealed haemorrhage may be massive.
- Tense, woody uterus + constant pain = classic sign.
- Placental abruption vs praevia → painful bleeding vs painless bleeding.
- Always stabilise mother before focusing on fetus.
- DIC risk is high → always monitor clotting + fibrinogen.
