
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Rubella (German Measles) Notifiable
Related Subjects: |Herpes Varicella-Zoster (Shingles) Infection |Chickenpox Varicella Infection |Varicella Cerebral Vasculopathy |Herpes Viruses |Herpes Zoster Ophthalmicus (HZO) Shingles |MonkeyPox |Mumps |Measles |Rubella (German Measles) |Epstein-Barr Virus infection
🤒 Rubella is usually a mild viral illness but has major consequences in pregnancy. If contracted in the first trimester, it can cause severe congenital anomalies including cataracts, heart defects, and sensorineural hearing loss.
📖 About
- Also called German measles (distinct from measles/rubeola).
- 🦠 RNA virus; incubation 14–21 days; epidemics occur every 10 years.
- 🌬️ Spread via respiratory droplets; peak incidence in teenagers and young adults.
- 💉 Vaccine-preventable (MMR); widespread immunisation has drastically reduced cases.
🩺 Clinical Presentation
- Often subclinical, but still contagious.
- 🌡️ Mild fever, malaise, conjunctivitis, coryza.
- 🤧 Lymphadenopathy (posterior cervical, auricular, suboccipital) is typical.
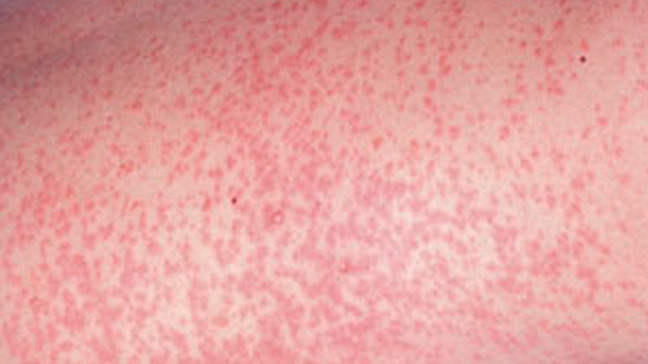
- 🌸 Maculopapular rash: pink-red, starts on face → spreads to trunk/limbs, fades by day 3–5.
- 🔴 Forchheimer spots: small petechiae on soft palate.
- 🕒 Infectious from 7 days before rash → 7 days after.
🌸 Rubella Rash
⚠️ Complications
- Pregnancy risk: Congenital Rubella Syndrome (CRS) if infection in 1st trimester.
- 🧠 Encephalitis (~1 in 5,000, mortality 30–50%).
- 🤲 Transient arthritis (esp. in adult women).
- 🩺 Transient hepatitis.
🤰 Rubella in Pregnancy
- CRS triad:
- ❤️ Congenital heart disease (PDA, VSD).
- 👁️ Ocular: cataracts, microphthalmia.
- 👂 Sensorineural hearing loss.
- Also: microcephaly, developmental delay, hepatosplenomegaly, bone lesions, interstitial pneumonia.
- 📅 First trimester = greatest risk; later infection is less damaging but still concerning.
🔎 Investigations
- Serology: Rubella IgM (acute infection), rising IgG titre (recent infection).
- Viral isolation from nasopharynx useful in pregnancy cases.
- A fourfold IgG rise between acute and convalescent samples confirms infection/reinfection.
💊 Management
- Prevention: MMR vaccination (two doses) = best protection.
- Preconception: Check rubella immunity in women planning pregnancy. Vaccinate if non-immune (contraindicated once pregnant).
- During pregnancy:
- Serology if exposed.
- Immunoglobulin sometimes considered, but limited efficacy at preventing CRS.
- Supportive care: No antiviral; manage with fluids, antipyretics, analgesia.
- CRS: Supportive treatment for complications – e.g., cardiac surgery, cochlear implants, cataract surgery.
💡 Exam tip: Think of rubella in a non-immune pregnant woman with rash + lymphadenopathy. CRS = classic triad of congenital heart disease + cataracts + hearing loss.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery