Related Subjects:
|Brain tumours
|Astrocytomas
|Brain Metastases
|Tuberous sclerosis
|Turcot's syndrome
|Lhermitte Duclos Disease
|Oligodendroglioma
|Acute Hydrocephalus
|Intracranial Hypertension
|Primary CNS Lymphoma (PCNSL)
|Astrocytomas
|Glioblastoma
🧠 Meningiomas are common, usually benign brain tumours that arise from the meninges. While slow-growing, their location can cause significant neurological symptoms.
📌 About
- Meningiomas account for ~30% of all primary intracranial tumours.
- More common in women aged 40–70 (♀:♂ ≈ 2:1).
- Most are benign (WHO grade I), but atypical (grade II) and anaplastic (grade III) variants are more aggressive.
- Can be solitary or multiple, especially in Neurofibromatosis type 2 (NF2).
⚡ Aetiology & Risk Factors
- Slow-growing, usually present for years before symptoms appear.
- Cause compression and displacement of brain tissue rather than invasion.
- Hormonal influence: oestrogen, progesterone, and androgen receptors explain higher female prevalence and growth in pregnancy.
- Risk factors:
- 📡 Prior head/neck radiation (decades later).
- 🧬 Genetic (NF2 mutation – merlin protein dysfunction).
- 🤰 Hormonal influences (pregnancy, HRT).
- Trauma (suggested but not strongly proven).
🔬 Pathology
- Originates from arachnoid cap cells in arachnoid granulations.
- Histological subtypes:
- Meningothelial – lobulated whorls (most common).
- Fibrous – spindle cells with collagen bundles.
- Transitional – features of both.
- Papillary/Rhabdoid – aggressive, poor prognosis.
- 🌀 Psammoma bodies (calcified concentric structures) often seen.
- IHC: Positive for EMA and vimentin.
📍 Common Locations
- Falx cerebri → leg weakness/numbness.
- Convexity → seizures, focal deficits.
- Lesser wing of sphenoid → visual loss, proptosis.
- Olfactory groove → anosmia, frontal lobe personality change.
- Posterior fossa → ataxia, vertigo, cranial nerve palsies.
- Spinal cord (intradural–extramedullary) → compressive myelopathy.
🩺 Clinical Features
- 📌 Often incidental – found on imaging.
- Symptomatic tumours may cause:
- Headache from ↑ICP.
- Seizures (especially cortical meningiomas).
- Focal deficits – motor/sensory loss, CN palsies.
- Cognitive/personality change (frontal lobe).
- Visual field defects (parasellar/optic compression).
- Gait disturbance (parasagittal/cerebellar tumours).
🧪 Investigations
- CT scan: Detects calcification, hyperostosis, bone involvement.
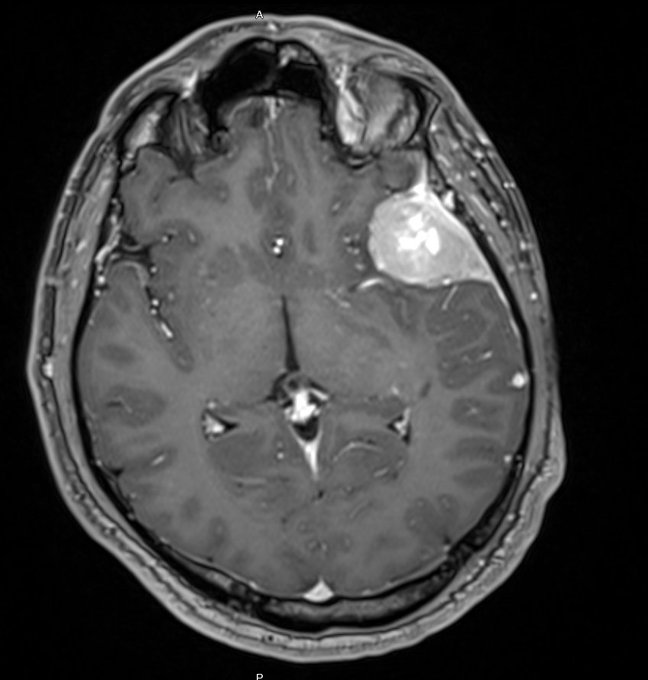
- MRI with contrast (gold standard):
- Extra-axial, well-circumscribed, strong contrast enhancement.
- Characteristic “dural tail” sign.
- Angiography: Defines vascular supply (useful pre-op).
- Biopsy: Histology for atypical/malignant lesions.
💊 Management
- Observation: Suitable for small, asymptomatic, slow-growing lesions (monitor MRI 6–12 monthly).
- Surgical resection: Mainstay for symptomatic/growing tumours. Goal = Simpson grade I resection (complete excision including dural base).
- Radiotherapy:
- Stereotactic radiosurgery (Gamma Knife) for small/inaccessible lesions.
- Fractionated RT for recurrent or malignant cases.
- Medical therapy:
- Anticonvulsants for seizures.
- Antiprogesterone agents (e.g. mifepristone) under study.
📈 Prognosis
- Grade I: Excellent with complete excision.
- Grade II/III: High recurrence → may need adjuvant RT/chemo.
- Outcome depends on:
- Location (surgically accessible vs skull base).
- Histological grade.
- Extent of resection (Simpson grade).
Enhancing meningioma with dural tail