Related Subjects:
|Subarachnoid Haemorrhage
|Perimesencephalic Subarachnoid haemorrhage
|Haemorrhagic stroke
|Cerebellar Haemorrhage
|Putaminal Haemorrhage
|Thalamic Haemorrhage
|ICH Classification and Severity Scores
🧠 About Pontine/Midbrain Haemorrhages
- ⚠️ Poor Prognosis: Brainstem haemorrhage carries a very high fatality rate, often ≥50%, due to involvement of vital respiratory and cardiovascular centres.
- 📉 Rarity: Represents a small fraction of all intracerebral haemorrhages (<10%), but outcomes are disproportionately severe.
- 🏥 Clinical Importance: Early recognition and rapid supportive management are critical; mortality is highest in the first 24–48 hours.
- Guideline Alignment: Management follows NICE stroke guidelines (NG128) and UK Stroke Association recommendations for acute ICH.
🩸 Vascular Anatomy
- Paramedian perforators: Supply the medial pons and midbrain; bleeds here often bilateral and rapidly fatal due to involvement of corticospinal tracts and respiratory centres.
- Lateral short penetrating arteries: Supply cranial nerve nuclei; haemorrhage may cause cranial nerve deficits (CN V–VIII), facial weakness, gaze palsy, hearing loss, vertigo.
- Long circumferential arteries (branches of AICA and SCA): Supply lateral tegmentum; bleeds often less severe, presenting with ataxia, sensory loss, and less life-threatening symptoms.
🧬 Causes
- 💢 Hypertension: Most common cause; chronic small vessel disease leads to paramedian perforator rupture.
- 🕸️ Arteriovenous malformations (AVM): Congenital vascular malformations prone to rupture.
- 🫀 Cavernous malformations (cavernomas): Low-pressure capillary clusters; bleeds usually smaller, sometimes better prognosis.
- ⚡ Other causes: anticoagulation, coagulopathies, amyloid angiopathy (rare in brainstem), trauma.
🩺 Clinical Presentation
- Severe/Classic: Sudden coma, quadriplegia or quadriparesis, pinpoint pupils (miosis), apnea, dysarthria, dysphagia, rapidly fatal.
- Cranial nerve involvement: CN V–VIII → facial numbness/weakness, diplopia, hearing loss, vertigo, dysphagia, dysphonia.
- Milder/Lateral: Ataxia, dizziness, nausea, vomiting, sensory deficits, tremor, nystagmus.
- Autonomic instability: BP fluctuations, bradycardia, respiratory irregularities, requiring ICU monitoring.
🔍 Investigations
- 🧪 Laboratory: Coagulation screen, FBC, U&E, electrolytes; rule out coagulopathy or thrombocytopenia.
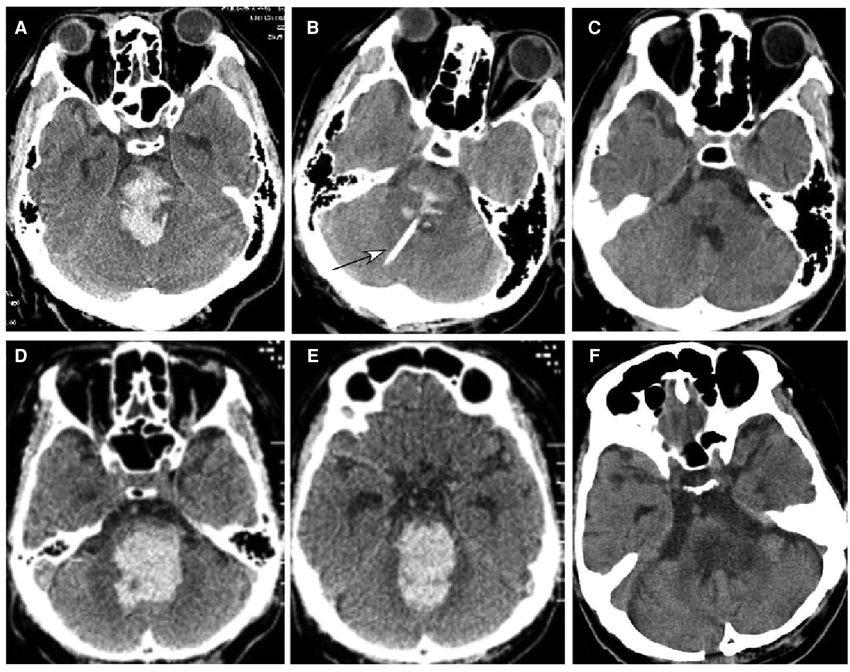
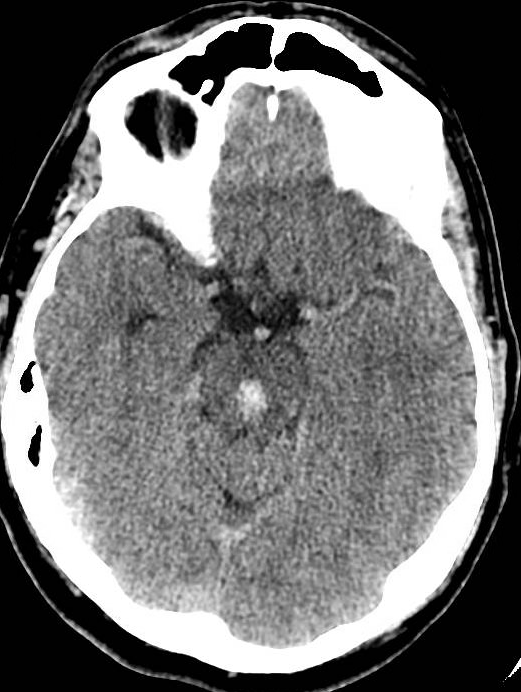
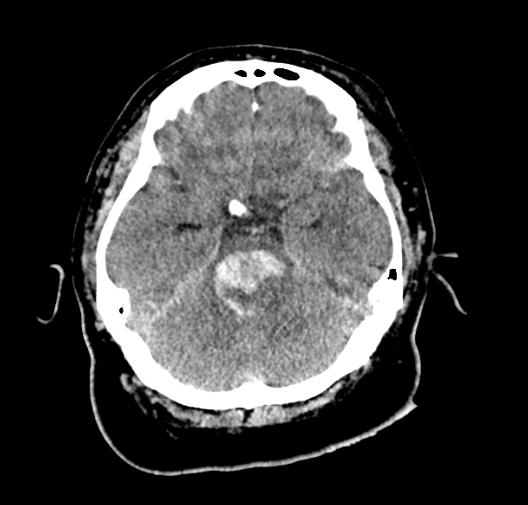
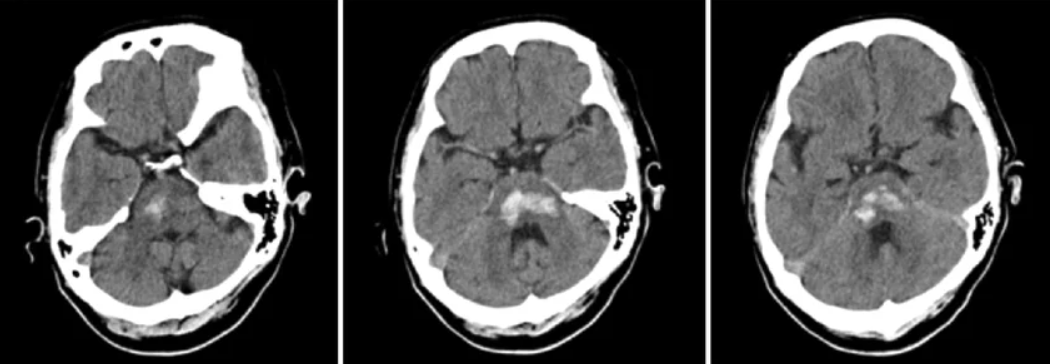
- 🖼️ Imaging: Non-contrast CT for rapid detection of haemorrhage; MRI brainstem (T2*/GRE) for microbleeds, cavernomas, or AVM detection.
- 🧲 Vascular studies: CT/MR angiography to identify AVM, aneurysm, or vascular malformations.
- ⚠️ Monitoring: Serial imaging if neurological status changes; ICP monitoring in severe cases.
⚖️ Management
- 🛑 Conservative/supportive: Mainstay due to surgical inaccessibility; includes airway protection, ventilation, and haemodynamic support.
- 🏥 ICU care: Maintain oxygenation, manage blood pressure per NICE stroke guidance (target SBP <140 mmHg if safe), prevent aspiration, and monitor for complications.
- 💊 Blood pressure control: Antihypertensives titrated carefully; avoid hypotension.
- 🧑🦽 Rehabilitation: Early neuro-rehab for survivors; physical, occupational, and speech therapy to maximise function.
- 🧑⚕️ Neurosurgical input: Consider only for decompression if superficial lateral brainstem haematoma or associated AVM/aneurysm; otherwise, surgery is rarely feasible.
- 🛡️ Prevention of recurrence: Strict vascular risk factor modification – control hypertension, diabetes, cholesterol, and smoking cessation.
📉 Prognosis
- High early mortality; survival heavily dependent on haemorrhage size, location, and initial level of consciousness.
- Survivors commonly have severe neurological deficits: quadriplegia, cranial nerve palsies, bulbar dysfunction, respiratory dependence.
- Prognosis improved with early recognition, optimal ICU care, and BP management.
📝 Notes
- 🩺 Primary prevention: aggressive hypertension detection and treatment reduces incidence.
- 🧑⚕️ Secondary prevention: identify and manage AVMs or cavernomas where feasible; regular imaging if high-risk lesions present.
- ⚠️ Alignment with guidelines: Follows NICE stroke guidelines and UK Stroke Association recommendations for ICH and ICU management.
💡 Exam Pearl: Sudden coma, quadriparesis, pinpoint pupils → classic pontine haemorrhage. Early ICU supportive care is critical; surgical intervention rarely feasible.
