
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Stroke Related Cerebral Perfusion
🧠 Physiology of Brain Perfusion
- 🧠 The brain weighs about 1.4 kg, which is only around 2% of body weight in a 70 kg adult. Despite this, it receives about 15% of the cardiac output, equivalent to roughly 750 mL/min of blood flow.
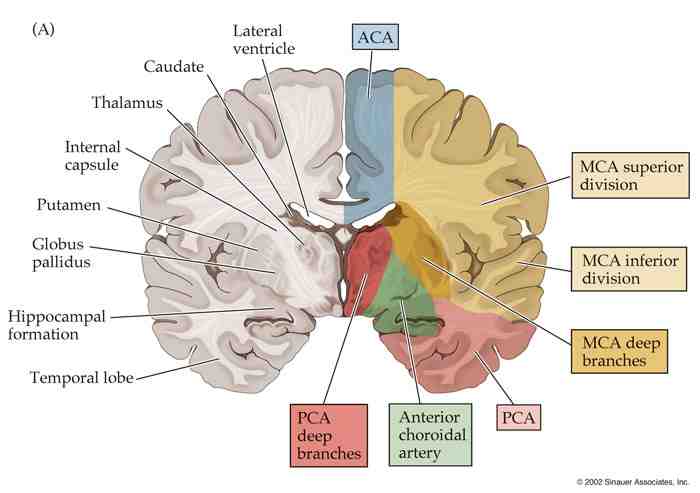
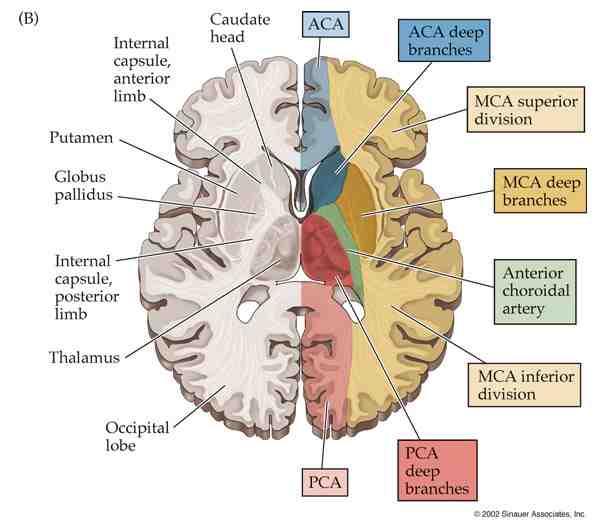
- 🩸 Cerebral perfusion is supplied by 2 internal carotid arteries and 2 vertebral arteries. Around two-thirds of flow comes from the anterior (carotid) circulation, while the vertebral arteries form the posterior circulation, supplying the brainstem, cerebellum, and posterior cerebrum.
-
🔄 The Circle of Willis connects the carotid and vertebrobasilar systems, providing a potential route for collateral circulation.
- Under normal circumstances, there is little physiological cross-flow because there is no major pressure gradient to drive mixing.
- 🚨 If an artery becomes narrowed or occluded, collateral flow may partly preserve perfusion, but often not enough to fully prevent ischaemia or infarction.
- 🧩 Grey matter receives substantially more blood flow than white matter, reflecting its much higher synaptic and metabolic activity. Cortical neurons are especially vulnerable to hypoxia, and irreversible neuronal injury may begin within only a few minutes of severe interruption of oxygen delivery.
- 🔥 The brain accounts for about 20% of total body oxygen consumption. It depends heavily on a constant supply of oxygen and glucose, with very limited energy reserves, so interruption of perfusion rapidly causes dysfunction.
🩸 Cerebral Blood Flow (CBF)
- ⚖️ Cerebral blood flow is tightly regulated by autoregulatory, chemical, and local metabolic mechanisms.
-
🌬️ Carbon dioxide is one of the most powerful regulators of CBF. Rising arterial PaCO₂ increases hydrogen ion concentration around cerebral vessels, causing vasodilation and an increase in CBF.
- As a rough rule, every 1 mmHg rise in PaCO₂ can increase cerebral blood flow by about 4%.
- So marked hypercapnia can dramatically increase cerebral perfusion and intracranial blood volume.
- 📍 Blood flow can also increase very rapidly in brain regions with increased neuronal activity. This is called neurovascular coupling. For example, voluntary movement of one hand rapidly increases perfusion to the contralateral motor cortex.
-
🛡️ Autoregulation helps maintain relatively constant cerebral blood flow across a wide range of systemic blood pressures by adjusting cerebrovascular resistance.
- In healthy adults, this usually operates across a mean arterial pressure range of about 50–150 mmHg.
- When blood pressure rises suddenly, cerebral arteries constrict to protect the distal microcirculation.
- When pressure falls, cerebral vessels dilate to preserve flow.
- If autoregulation fails, cerebral perfusion becomes pressure-dependent, increasing the risk of ischaemia or hyperperfusion injury.
-
😮💨 Hypocapnia, usually caused by hyperventilation, causes cerebral vasoconstriction. This reduces CBF and can lower intracranial pressure (ICP).
- This principle is sometimes used in critical care for short-term control of raised ICP.
- However, excessive hypocapnia can reduce cerebral perfusion too much and worsen ischaemia, so it is used cautiously.
- 📉 Severe hypoxaemia can also increase cerebral blood flow, but this effect usually becomes important only when oxygen tension falls substantially. Similarly, severe hypoglycaemia threatens brain function because the brain relies heavily on glucose as its main fuel.
🚨 Strokes and Perfusion
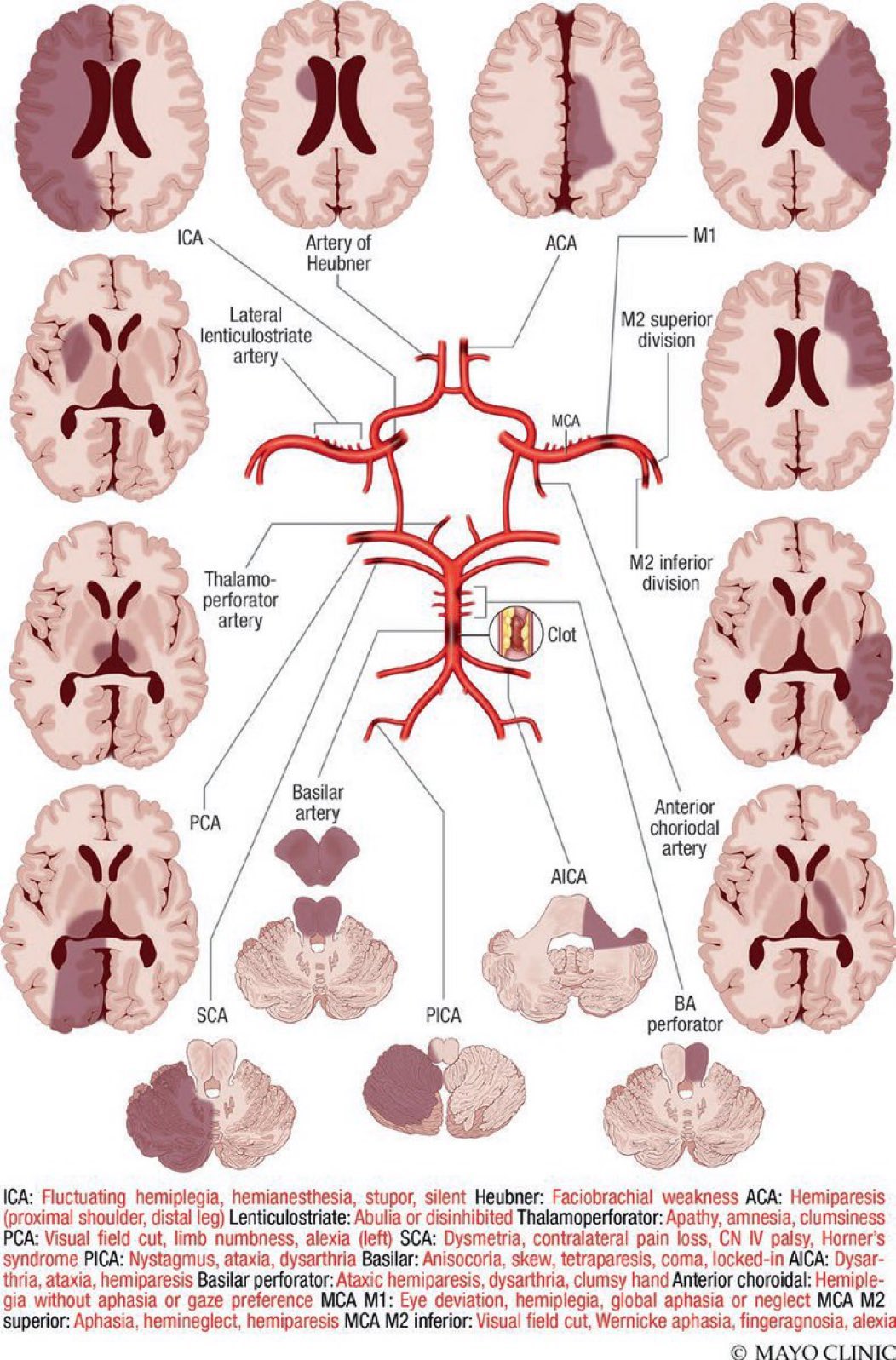
🧠 Stroke usually results from sudden interruption of cerebral perfusion, most commonly due to arterial thrombosis or embolism. Reduced or absent blood flow deprives brain tissue of oxygen and glucose, leading first to ischaemia and then to infarction if perfusion is not restored quickly.
🩸 In ischaemic stroke, the core infarct is surrounded by potentially salvageable tissue known as the ischaemic penumbra, where blood flow is reduced but not yet below the threshold for irreversible injury. This is the physiological basis for urgent reperfusion therapies such as thrombolysis or thrombectomy.
💥 In haemorrhagic stroke, rupture of a cerebral vessel causes direct tissue injury, local compression, impaired perfusion, and often a rise in intracranial pressure. So although the mechanism differs, the final common pathway is still neuronal injury from disrupted perfusion and secondary damage.
💡 Key summary:
🧠 The brain is a small organ with an enormous metabolic demand.
🩸 It depends on continuous blood flow for oxygen and glucose delivery.
🌬️ CO₂ strongly alters cerebral vessel diameter, while autoregulation buffers the effects of changing blood pressure.
🚨 When perfusion falls below critical levels, brain tissue rapidly becomes ischaemic and can infarct within minutes.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery