
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Air Embolism ✅
Related Subjects: |Acutely ill patient |Distributive Shock |Hypovolaemic or Haemorrhagic Shock |Obstructive Shock |Septic Shock and Sepsis |Shock (General Assessment) | Air Embolism | Fat Embolism |Acute Anaphylaxis
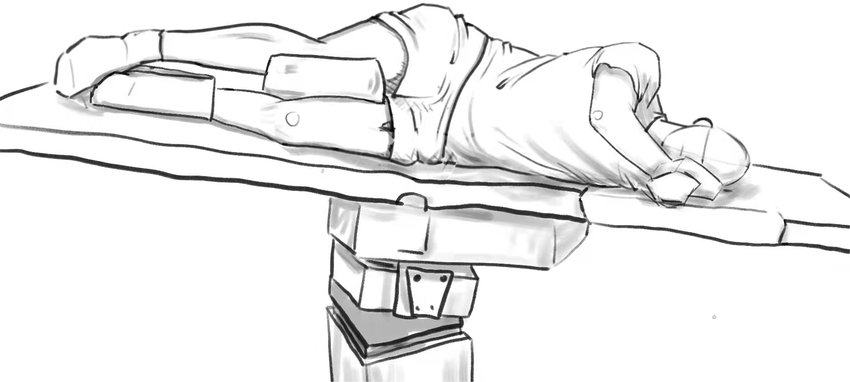
💨 Air Embolism occurs when air bubbles enter the bloodstream, obstructing circulation. This can happen during surgery, trauma, medical procedures, or diving accidents 🏊♂️. Severity depends on volume of air and site of obstruction. Clinical features include acute neurological deficits (e.g., hemiparesis, seizures), cardiovascular collapse, and hypoxia. 📌 Immediate Positioning: Left lateral decubitus + Trendelenburg (head down, left side down) → traps air in the right ventricular apex, slowing systemic entry. Give high-flow oxygen: 10–15 L/min via non-rebreather mask or up to 60 L/min via high-flow nasal cannula.
📌 About
- ⚙️ Mechanism: Air enters venous or arterial circulation → obstructs blood flow → impaired perfusion.
- 🫀 Venous Air Embolism (VAE): Air reaches right heart → pulmonary artery obstruction → hypoxia, RV strain, cardiovascular collapse.
- 🧠 Arterial Air Embolism (AAE): Can reach brain, heart, kidneys → stroke, MI, multiorgan injury.
- 🤿 Diving/Decompression: Rapid ascent → nitrogen bubbles mimic air embolism (decompression sickness).
- ⚠️ Severity: Small volumes (0.5–1 mL in coronary/cerebral arteries) can be fatal; >50 mL venous air may cause cardiovascular collapse.
🔬 Pathophysiology
- 🩸 Venous entry favoured when site is above right atrium → negative pressure sucks in air.
- 🚪 Arterial embolism may arise via pulmonary barotrauma or paradoxical embolism through PFO/ASD.
- 🧠 Cerebral & coronary arteries most vulnerable → stroke-like deficits, MI.
📋 Causes
- 🩻 Surgical: Neurosurgery, cardiothoracic surgery, central line insertion/removal.
- 🪓 Trauma: Penetrating chest/neck injuries or fractured veins.
- 💉 Central Lines & Catheters: Most common iatrogenic cause.
- 🤿 Diving Accidents: Poor decompression control → overlap with nitrogen embolism.
- 💨 Positive Pressure Ventilation: Barotrauma → alveolar-vascular air entry.
🩺 Clinical Features / Red Flags
- 😮 Dyspnoea, hypoxia, cyanosis
- ❤️ Chest pain, arrhythmias
- 🧠 Neurological: dizziness, seizures, confusion, focal deficits, hemiparesis
- 📉 Hypotension, obstructive shock
- 💔 Cardiac arrest in severe cases
🔎 Investigations
- 🧪 ABG → hypoxia ± metabolic acidosis
- 📈 ECG → RV strain, tachycardia, ST changes
- 🩻 CXR → non-specific, may show pulmonary oligemia
- 🫀 TEE → sensitive for air bubbles in RA/RV (especially intraoperative)
- 🧪 Consider blood tests to rule out alternative causes (e.g., PE, stroke)
🩺 Differentials
- 🫁 Pulmonary embolism
- 🧠 Stroke / TIA
- ❤️ Myocardial infarction
- 🫁 Tension pneumothorax
- 💔 Cardiac tamponade
🚨 Complications
- 💔 Cardiac arrest / obstructive shock
- ❤️ Myocardial infarction
- 🧠 Hypoxic brain injury / stroke
- 🫁 ARDS & respiratory failure
🛡️ Prevention
- 🏥 Careful central line insertion/removal; use air filters where possible
- 🤿 Divers → controlled ascent, decompression stops
- 💉 Maintain air-tight connections, patient positioning during line manipulation
⚕️ Management
- 🔄 Resuscitation: ABCs, high-flow oxygen (10–15 L/min NRB or 60 L/min HFNC)
- 🛏️ Position: Left lateral decubitus + Trendelenburg
- 🤐 Intubation/ventilation if severe hypoxia
- 💧 Fluids ± inotropes to maintain preload & cardiac output
- 💉 Aspiration via central line if RA accessible (intraoperative / ICU setting)
- 🌊 Hyperbaric Oxygen Therapy (HBOT) → gold standard for cerebral or cardiac involvement; ideally <8 hours from onset
- 🔪 Open chest aspiration → rare, intraoperative emergency
💡 Teaching Pearl: Early recognition + positioning + high-flow oxygen can reverse neurological deficits and prevent mortality. Neurological recovery may be slow but often improves with prompt intervention.
📉 Prognosis
- ⏱️ Dependent on speed of recognition and treatment
- ✅ Early intervention → good functional recovery
- ❌ Delay → permanent neurological injury or death
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery